The Biology of a Pandemic
The COVID-19 pandemic which began in late 2019 has been truly devastating event that has caused not only widespread illness and death, but disruptions in virtually all human activities.
COVID-19 is the disease caused by the coronavirus SARS-CoV-2. The Coronaviruses are a large family of viruses that can infect mammals and birds causing diseases that range from mild colds to acute respiratory syndromes (hence SARS) and death. The term "coronavirus" comes from the spike proteins that radiate from the external envelop (corona=crown).
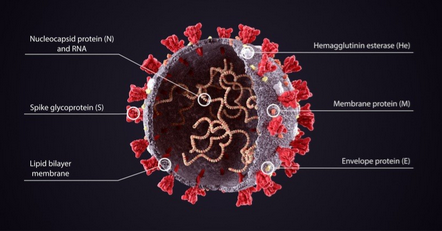
The envelope consists of spike proteins sticking out of a lipid shell that encloses the single RNA genome and some proteins.
The virus enters the body through the mouth or nose, and fuse with a specific proteins on the surface of a cell and inject their RNA genome into the cell. The cell's ribosomes translate the virus's RNA into proteins including RNA polumerase which transcribe the virus's RNA, making more RNA copies that are translated into proteins and more copies of the genome. Then the genome and proteins combine to make a new virus packaged into an envelope formed from the cells membranes. Newly formed cells travel to the cells surface and are released outside the cell, where they can infect other cells or leave the body in mucus and saliva droplets.
By the Numbers
Death Rate
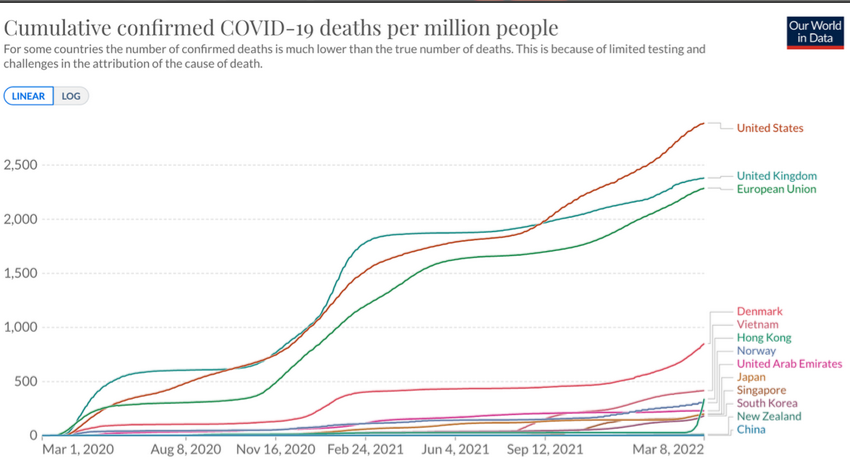
The COVID-19 pandemic emerged in 2019 and as of April 2022 is estimated to have caused illness in 500 million people globally and killed more than 6 million. Note how widely the death rate varied from country to country and how the rate declines and surges due to mutations of the viral genome. The factors responsible for these variations are not completely understood, but several major factors have been identified.
Basic Reproductive Number (R0)
Viruses differ in their inherent contagiousness and and in the absence of any preventive measures the contagiousness of a virus or bacterium is estimated as a quantity called R0 ("R naught").
R0 is a measure of the average number of new cases caused by an infected person in a population with no immunity.
Ex. If R0=3 one infected person would infect 3 more people to become infected on average. Each of those 3 infect 3 more and etc, resulting in an exponential increase.
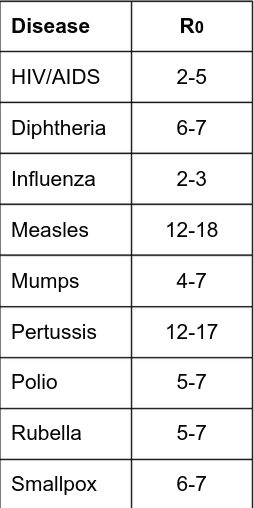
At the beginning of the pandemic everyone was susceptible and early estimates of R0 were around 2.2-2.7; causing a rapid increase in cases.
The Effective Reproductive Number
The basic reproductive number was relevant at the beginning of the pandemic because no one was immune and no control measures had been instituted. However the reproductive number has changed over time, partly because people who were infected and have immunity for a while. In addition, the probability of transmission of a respiratory virus or bacterium may be influenced by other factors such as:
- Immune Status
- Frequency of contact with others
- Duration of contact
- Proximity of contact
- Ventilation
- Wearing an effective mask
- Hand Washing
- Climate and seasonal variation
- The duration of disease in infected persons
- COVID testing and contact tracing
- Isolation and Quarantine
- Availability and utilization of effective vaccine
Seasonal variation is beyond our control, but the other known factors provide opportunities for interventions that can reduce the effective reproductive number.
If the effective reproductive number remains greater than 1 an epidemic or pandemic will continue. If interventions reduce the effective reproductive number below 1 and keep it there it will eventually disappear.
In absence of any intervention, diseases like COVID-19 can spread rapidly in a susceptible population.
The US and most of Europe experienced much higher morbidity and mortality rates compared to countries such as China, Japan, South Korea, and New Zealand which adopted rigorous social distancing measures. These measures prevented the early exposure surge and when relaxed the rates of infection rebounded.
Vaccines and Heard Immunity
If this can be achieved, the opportunities for transmission to susceptible people become diminished to the point that propagation of the virus cannot be sustained. When this is achieved, even susceptible persons enjoy a significant degree of protection.
The fraction of a population that must be immune (by being vaccinated or by recovering from infection) to achieve heard immunity can be estimated by [1 - (1/R0)]
Ex. For a typical strain of influenza A with R0 = 2.5, it would be desirable to vaccinate at least 1 - 1/2.5 = .6 or 60% of the population. Since R0 for COVID was in this range early in the pandemic, this was the goal that many articulated when vaccines began development.
Highly effective vaccines against COVID-19 became available in Dec 2020. Many people were eager to get it at first, but after a while vaccinations slowed due to vaccine hesitancy. As of April 2022, only ~66% of the US was fully vaccinated. This would have been sufficient if the R0 was still 2.4 but unfortunately mutations produced more transmissible strains such as the Delta strain with R0=5.08, and Omicron with 8.2. Achieving herd immunity against Omicron would theoretically require a vaccination rate of 88%.
Testing, Case Investigation and Contact Tracing
Many people infected with SARS-CoV-2 have minimal or no symptoms but can still transmit the disease to others.
In addition to promoting vaccination, another important strategy is abundant testing to identify symptomatic and asymptomatic cases in order to isolate them until they are no longer effective. Also, contacts of infected people should be traced and counseled regarding quarantine and what steps to take if symptoms develop.
Viral Mutations
When viruses replicate, random mutations occur occasionally. These may increase or decrease the transmissiblity or adverse effects of the virus, or have no effect. The more a virus replicates, the more likely that strains with altered properties occur. One consequence of not controlling the pandemic quickly is that viral replication continued at a staggering rate that is increased the probability of generating more transmissible strains.
COVID-19 Accentuates Inequities
Health equity means equal distribution and access to health resources for all people. It is strongly influenced by social determinants of health such as neighborhood, health care, work conditions, income, wealth, and education.
The CDC notes some racial and ethnic groups have been disproportionately effected by COVID-19 due to longstanding disparities in these determinants. Many politicians are noting that black people have more underlying medical conditions but they're not explaining why. They blame the choices made by black people or poverty or obesity - but never racism.
Communities of color are often redlined into housing with crowded neighborhoods with less access to public transportation, nutritious food and quality health care. These groups are also less likely to have health insurance and access to care. In addition, they disproportionately work in "essential" non-remote work settings such as health care, factories, food production, sales and public transportation. These workers generally also have lower incomes, less wealth, less paid sick leave, and more debt.
Medical and public health institutions have repeatedly violated the trust of communities of color through historic injustices including mistreatment and racism within public health and healthcare, leading to a well-earned skepticism of new interventions such as the COVID-19 vaccines. It was initially assumed people of color were accessing vaccines less but as of April 2022 this trend has changed, some communities of color have high vaccination rates than their white neighbors.
The life expectancy declined in all income groups during the pandemic but the poorest 20% which already had the lowest life expectancy had the greatest decrease.
No Comments