Non-Inferiority in Clinical Trials
Usually clinical trials should show if a new treatment is superior to placebo or no treatment, but as we've previously discussed it is not always ethical to give out a placebo when an effective treatment has been identified.
The goal of non-inferiority trials is to to demonstrate a new treatment (T) is NOT inferior (no worse than) the best available treatment (C), given the effect of the active control (compared to placebo or no treatment) has already been established.
Non-Inferior = Not Unacceptably Worse
In practice non-inferiority trials assess:
- If T is not necessarily more efficacious (superior) than C
- If T could be not as effective as C, but could have potential ancillary benefits:
- Lower procedural risks (safety)
- Less side effects
- Improved convenience
- Favorable costs
- Non-inferiority margin: How much worse we are willing to accept T compared with C
Hypothesis Testing
H0: πT - πC <= -δ (inferior)
HA: πT - πC > -δ (non-inferior)
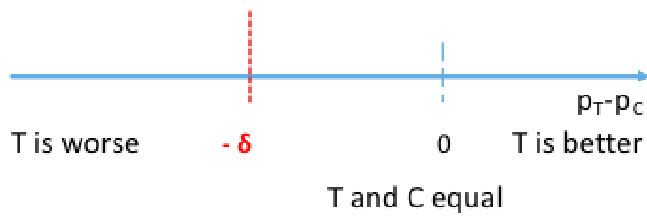
π represents the population level experimental and control proportions/risk of outcome
δ is the non-inferiority margin
Rejecting the null means non-inferiority is met, failing to reject the null means the new treatment is inferior. Both non-inferiority and superiority are met if T falls above the 'T and C' are equal point.
The null can also be rewritten as πT + δ <= πC, which is used in SAS
The FDA requirement for non-inferiority is alpha=.025.
Computing the 95% confidence interval for the difference in πT - πC we would reject the null when the CI's lower boundary is greater than -δ.