Foundations of Public Health
PH700: History, philosophy and core functions of public health
- Foundations of the Profession and Science of Public Health
- History of Public Health
- What is Public Health?
- Philosophy and Ethics in Public Health
- Evidence-Based Public Health
- Qualitative Reseach
- Trends in Morbidity, Mortality and Behaviors in the US
- Biological Foundations for Public Health
- Infectious Agents
- The Biology of a Pandemic
- Respiratory Health
- DNA, Heredity and Drug Resistance
- Cancer
- Heart Health
- Factors Related to Human Health
Foundations of the Profession and Science of Public Health
History, philosophy, and conceptual foundation of public health in the US
History of Public Health
Methods of preventing disease go back many centuries. Concepts of disease were crude and often based on anecdote. Some recommendations and practices were ineffective, if not even harmful to health such as bloodletting.
In the mid-1800's there was a hygiene movement, particularly in the UK, with focus of improvements of cleanness and well-being of the poor. Additionally, at the end of the 19th century germ theory became accepted.
Learning Objectives:
- Explain the evolution of concepts about cause and prevention of disease
- Understand the importance of studying the factors associated with outcomes in a systematic way in human populations.
- Discuss some of the major historical figures and events that played a role in evolution of public health and epidemiology
- Describe the overall structure of the public health system in the US today
Early Concepts of Disease
10,000 years ago when humans were hunter-gatherers and lived in small, nomadic groups accumulating waste and contamination wasn't a problem. Early concepts of disease revolved around superstition, myths and religion (bad spirits, Pandora's box, etc).
The agricultural revolution provided more secure supply of food and enable expansion of population. People often lived off one or two crops, often lacking protein and vitamins. The domesticated animals provided food and labor, but also carried diseases that could be transmitted to humans. Waste accumulation attracted rodents and insect vectors and with people living in larger groups there was a greater opportunity for transmission of diseases.
The first concept of disease not founded on superstition was the Hippocratic corpus; A Greek concept that disease is caused by an unbalance of the environment or natural forces, and Blood, Bile, Phlegm, and Melancholy must be kept equal within the body. Although the concept clearly incorrect by today's medical standards, Greek doctors would prescribe changes in diet and lifestyle. It also became the rational for bloodletting, which continued for many centuries despite lack of evidence.
The Bubonic Plague
The bubonic plague caused by a bacteria that lives in the intestines of fleas. Fleas were the vector and rats were a reservoir for the bacteria that could easily transmit the disease. Occasionally, an infected flea could jump to a human and infect them directly. Causing dark, tender, swollen nodules. Symptoms also included headache, and delirium and was fatal in about 60% of cases.
Starting in 1347 Europe experienced waves of the plague which lasted until the late 1700's. It was believed to have originated in Asia and traveled along trade routes to the black sea. 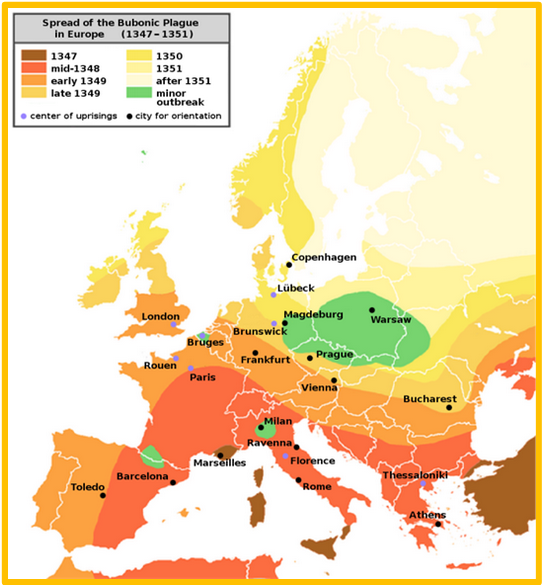
The most popular explanation was that it was caused by miasmas - invisible vapors which emanated from swamps or cesspools and floated around in the air where they could be inhaled. One pope kept fires burning on both sides of the room to counter miasmas. Plague doctors kept herbs and flowers in a beak-like mask to ward of miasmas. Of course these were all ineffective as it was spread by flea bites. In a sense the real cause of transmission was population density and waste stagnation, which attracted rats with the fleas that carried the plague. Later the pneumonic form of the plague caused people to cough up blood and could spread by inhalation.
One might blame the lack of preventative measures and knowledge about transmission on the primitive understanding of medicine, however this wasn't due to a lack of technology but the fact that humans had not come up with a structured way to think about disease. There were theories about how the plague spread and how to prevent it, but no tests were ever done through observation of large groups of people. The idea of studying groups of people to identify risk factors and disease outcomes had not yet evolved. The lack of a systematic way of testing possible associated between exposures and outcomes was the major factor that prevented advances in understanding the causes of disease and development of effected treatment/prevention.
The black plague still exists today, and kills a few thousand people every year due to anti-biotic resistant strains. However, when identified early it is curable.
Quarantine and Isolation
The concept of quarantine dates back to the early 1400's and the black death. In Italian Qaurintina means 40 days. Travelers and merchandise thought to have been exposed would isolate for a set period of time. This practice persisted until the 19th and 20th century. Isolation is separating someone who has the disease from the rest of the population, which was useful in cases like SARS where the infected is only contagious when symptoms are present. Quarantine is separating someone from the population who might have been exposed, e.g. COVID-19 since one could be contagious without symptoms.
Public Health in the US
Events in the US paralleled those of the UK as the population moved from an agricultural to an urban and industrial way of living.
Timeline 1800s
- 1798: Congress passes the Act for the Relief of Sick and Disabled Seaman and authorizes the formation of US Marine Hospital Service (MHS), a forerunner of the Public Health Service. Seamen were taxed 20 cents per month to fund physicians and support the network of hospitals. The tax was abolished in 1884 and replaced with a levy on merchant ships, then after 1906 funds were allocated by congress.
- 1799: Castle Island in Boston Harbor was chosen as the temporary site for the first marine hospital. Dr. Thomas Welsh was named physician in charge.
- 1799: Boston establishes the first board of health and the first health department in the US. Paul Revere is named as the first health officer.
- 1800: Dr. Ben Waterhouse introduced smallpox vaccination to the US
- 1804: The Boston Marine Hospital is established in Charlestown, Boston. Dr. Ben Waterhouse was appointed physician in charge from 1807-1809
- 1842: MA Legislator Lemuel Shattuck established the first US system for recording births, deaths and marriages. This became the model for states across the Union. Among his contributions were a standard nomenclature for disease; establishment of a system for recording mortality data by age, sex, occupation, socioeconomic level, smoking, and drinking.
- 1849: The MA legislature appointed a Sanitary Commission to prepare a plan for reporting a 'Sanitary Survey of the State' with Shattuck as Chief Commissioner and author. While well-received by the New England Journal of Medicine, the 50 recommendations in the report went ignored. 20 years later the Board of Health based their plans on Shattuck's recommendations.
- 1870: The Marine Hospital Service was reorganized to change the general character of the service. Medical officers, called surgeons, were required to pass entrance examinations and wear uniforms. In 1889 the medical officers were given titles and pay corresponding to the Army and Navy grades. The goal was to create a professional, mobile health corps free from political favoritism to deal with health needs of a growing nation.
- 1874: MA State Board of Health instituted a voluntary plan for weekly reporting of disease by physicians.
- 1884: MA passes legislation requiring the reporting of "diseases dangerous to the public health" and imposes fines for not reporting.
- 1887: A "Hygienic Lab" was established at the marine hospital on Staten Island to aid in the diagnosis of infectious disease among passengers of incoming ships. It eventually moved to Washington DC and became the National Institutes of Health.
- 1891: The Immigration Act of 1891 required all immigrants entering US be given health examination by PHS physicians. All "idiots, insane persons, paupers or people suffering from disease and criminals" were excluded. Ellis island in New York Harbor was the largest inspection site.
- 1894: The first epidemic of polio strikes the US.
Timeline 1900s
- 1900: Estimates suggest HIV was transmitted from monkeys to humans as early as 1884-1924 but was either unrecognized or failed to initiate human to human transmission.
- 1902: US Congress expanded scientific research at Hygienic Laboratory and gave it a definite budget. Marine Hospital Services were renamed Public Health and Marine Hospital Services (PHMHS).
- 1906: Congress passed the Federal Meat Inspection Act requiring the Department of Agriculture to inspect mean entering interstate commerce. They also passed the Food and Drugs Act that forbade adulteration and misbranding of foods, drinks, and drugs, but contained few requirements to insure compliance.
- 1910-16: The working environment and effect on worker's health became a major area of study for the Public Health Service
- 1918: The influenza pandemic of 1918 is believed to caused 25-50 million deaths worldwide.
- 1925: All states begin participating in national reporting of disease
- 1938: Congress passes Federal Food, Drug, and Cosmetic Act of 1938, and major changes were made in 1954, 58, and 60. Today the law requires manufacturers to provide scientific proof of a drug's safety and prevents mislabelling of products. Enforcement of these laws is the mission of the FDA.
- 1952: Polio cases surge in the US. Early testing of Jonas Salk's vaccine is encouraging
- 1953: Under President Eisenhower Congress created the Department of Health, Education and Welfare (HEW)
- 1954: A large scale clinical trial of the Salk vaccine begins.
- 1964: Sugeon General Luther Terry concerned a panel of experts to review the impact of smoking on health.
- 1970: The Occupational Safety and Health Act was passed by Congress and OSHA was founded in 1971
- 1970: EPA established
- 1979: HEW's educational tasks were transferred to the new Department of Education and health tasks to the new Department of Health and Human Services (HHS)
- 1979: Smallpox is declared eradicated by the World Health Organization. Last known case was 1977 in Somalia
- 1980: President Jimmy Carter signed the Comprehensive Environmental Response, Compensation and Liability Act (CERCLA or Superfund) to give the EPA authority to clean up hazardous waste spills
- 1981: Dr. Michael Gottlieb and his associates reported on four previously healthy young men who developed Pnewmoncystis carinil pneamonia. This was monumental in bringing attention to the HIV/AIDS epidemic.
Ideas About Health
Examples of a few key players who influenced how we think about health and disease and it's determinites:
- Girolamo Fracastoro (1546) - Italian physician, poet and astronomer who wrote about "disease seeds" carried by wind. In a way he was proposing germ theory 300 years before its formal discovery, though similar speculation had been made by Roman scholar Marcus Varro had been made in 1st century BC.
- John Graunt (1662) - Around 1592 parish clerks in London began recording deaths. In 1662 Graunt, as a member of the Royal Society of London, summarized the data from the Bills of Mortality in a publication called "Natural and Political Observations Mentioned in a Following Index, and Made Upon the Bills of Mortality". This publication made a variety of observations regarding common causes of death, higher death rates in men, season variation and the fact some diseases had constant death rates. He also estimated population size and growth and was the first to construct a "life table".
- Van Leeuwenhouk (1670s) - In 1665 Robert Hooke devised a compound microscope and discovered plant cells, coining the term "cells" in his book Micrographia. Leeuwenhouk of Holland was considered the father of microscopy. While working in a dry goods store and using magnifying glasses to inspect the quality of cloth he discovered new methods to achieve increased magnification up to x270. He was the first to see bacteria (1674), yeast, protozoa, sperm cells, and red blood cells.
- John Pringle (1740s) - A Scot who served as physician general to the British forces during the war of Austrian Succession. In 1752 he published "Observations on the Diseases of the Army" in which he proposed a number of measures to improve health of soldiers such as hospital ventilation and camp sanitation. He wrote extensively on the importance of preventing typhus, which he incorrectly believed was caused by filth (it is caused by bacteria and carried by lice). He also coined the term "Influenza".
- James Lind (1754) - A Scottish navel surgeon who studied Scurvy in sailors and conducted what may have been the first clinical trial in 1754, by treating Scurvy infected sailors with a variety of treatments and correctly finding that citrus fruits cured the illness. Although he was correct in the cure, he was wrong about the cause of the disease, which was caused by vit C deficiency.
- Broussais and Louis (1754) - Broussais was a prominent Parisian physician and a strong proponent of bloodletting. His vigorous use of leeches during a cholera epidemic in Paris substantially contributed to the mortality rate. Louis was a contemporary of Broussais who believed numerical methods to evaluate treatment and discovered bloodletting was ineffective. Since bloodletting was embedded in medical practice his findings were largely dismissed.
- Ignaz Semmelweis (1840s) - Hungerian physician who practiced in the maternity department in Vienna in the 1840s. Post-partum sepsis was a common occurrence nearly always fatal and of unknown cause at this point. There were two different maternity wards, one attended by midwives and one attended by medical students. The medical students often came directly from handling corpses without washing their hands. He was the first to suggested all students wash their hands with chlorinated water and as a result the mortality rate plummeted, though some still ignored the findings.
John Snow: Father of Epidemiology
In the 1800s there were large outbreaks of Cholera in America and Europe killing thousands of people. John Snow was a physician from London who studied Cholera for many years, and is credited with solving a outbreak in 1854. The theory on Cholera transmission was measimas or person to person contact. Snow began examining the victims and found symptoms were always related to the gastroinstestinal tract and reasoned that if it were spread by bad air there would by pulmonary symptoms so transmission was more likely to occur by food or water consumption.
Many Londoners received their water from hand pump wells that were located throughout the city and two private companies in particular pumped water from the Thames river to the areas primary effected by cholera. Of course, few people believed Snow since he couldn't actually prove there was something in the water. He ended the epidemic in 1854 by removing the handle to the infected water pump himself. Cholera remains a problem in countries with underdeveloped sanitation and water routes, such as Haiti. In these locations it is more realistic to vaccinate for cholera than fix the entire system.
The Sanitary Idea
In a way modern public health, i.e. as a function of government, comes from France and Britian around 1850-1875 in the wake of the consequences industrial revolution. However the circumstances that propelled the development of public health as a discipline, such as the importance of the size of a population in measuring the influence and power of a state. This crude notion made the idea of "numbering the people" important. John Graunt's office was the first of it's kind to mandate the recording of births, marriages, deaths. William Farr was the first Chief Statistician. The General Registrar's Office established the importance of surveillance with respect to health.
Another contributing factor was the start of the enlightenment, which embraced democracy, citizenship, reason, rationality and the social value of intelligence. One theme was the reduction of mortality and improvements to health had an economic value to society, healthy workers were able to contribute more. Utilitarianism, or the idea that one can measure the amount of evil by the misery created or relieved by an action, provided underpinnings for public health.
Health and Class
In 1842 Sir Edwin Chadwick, a social reformer, published a report entitled "Report into the Sanitary Conditions of the Laboring Populations of Great Britain proving that life expectancy is much lower in towns than in the countryside. He argued that it was possible for government to improve people's lives through reform and a healthier population would work harder and cost less to support. He concluded what was really needed was not more doctors but civil engineers to provide drainage of the streets and more efficient ways of delivering clean water and removing sewage. These ideas contributed to the idea that public health was a legitimate concern of government and led to the creation of legislation and government offices.
What is Public Health?
The many factors that contribute to disease and health, or determinants, are complex and often break down to genetic, environmental and lifestyle factors. In addition Public Health is a multi-disciplinary enterprise that requires expertise in biology, pathology, environmental science, sociology, psychology, government, medicine, statistics, communication, and more to truly understand.
Someone who is overweight and smokes might require a expensive heart surgery to prolong their life. However, public health is about the interventions that prevent disease from occurring in the first place, so the benefits tend to be less obvious. The prevention of disease not only prolongs life, but improves the quality of life. In a sense public health is the epidemic that didn't happen, or the heart disease that didn't developed. Successful public health is the sum of the adverse health outcomes that never occurred.
Learning Objectives:
- List and describe the three core functions of public health
- Expand on the three core functions of public health and discuss how they relate to the 10 essential functions of public health
- Define and give examples of primary, secondary, and tertiary prevention of disease
- Discuss modern concepts of population health
- Briefly explain how "Public Health 3.0" differs from earlier approaches.
- Explain the rationale and approach of Health Impact in 5 Years (HI-5)
- Outline the overall structure of global public health
- Outline the overall structure of US public health
Primary, Secondary, and Tertiary Prevention
The goal of primary prevention is to prevent healthy people from becoming ill. While that sounds easy, it often creates ethical conflicts when healthy people are asked to take additional steps to prevent developing disease (i.e. vaccination, exercise, smoking).
Secondary prevention consists of screening for disease in order to find sub-clinical disease and treat it in the hope that earlier treatment will provide reduced harm or cure (e.i. cancer screening, blood pressure test for hypertension, routine urine and blood analysis).
Once an individual has been diagnosed and treated for a disease, subsequent efforts to reduce effects are regarded as tertiary prevention (i.e. cardiac rehabilitation after a heart attack, exercise and weight loss for people who developed type 2 diabetes).
International Public Health Organizations
The World Health Organization (WHO) was created in 1948 by the UN as the global health authority that would coordinate and guide health policy, practice, research, and surveillance in participating countries. The headquarters is located in Geneva, Switzerland. The director general is appointed by the World Health assembly which consists of representatives from participating countries.
The core functions of the World Health Organization are:
- Providing leadership on matters critical to health and engaging in partnerships where joint action is needed.
- Shaping the research agenda and stimulating the generation, translation and dissemination of valuable knowledge.
- Setting norms and standards and promoting and monitoring their implementation.
- Articulating ethical and evidence-based policy options
- Providing technical support, catalyzing change, and building sustainable institutional capacity.
- Monitoring the health situation and assessing health needs.
The WHO oversees 6 region and each of these interacts with the national public health agencies of it's member nations. 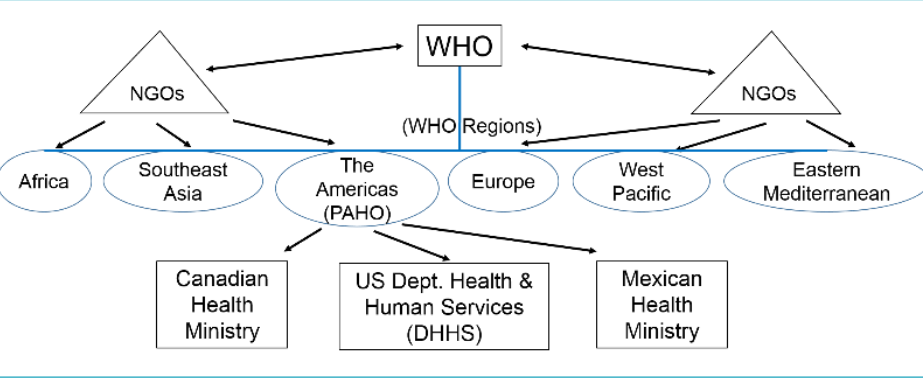
Non-Governmental Organizations (NGOs)
NGOs are private organizations that are not part of a particular government, though they often partner with governmental or inter-governmental organizations. They can be supported by public or private funding, and thus may be supported by government but not governed by them. NGOs are important to countries to provide programs to countries that do not have them such as HIV prevention, clean water allocation, and disaster relief. Ex. Red Cross, CARE for Europe.
Public Health in the US
In some respect Winslow's definition of public health is still correct today but in the US the focus has shifted over the last several decades.
In 1988 The institute of Medicine issued a report entitled "The Future of Public Health" which concluded the US public health system needed refocusing because there was a lack of clarity regarding its roles and responsibilities. The report introduced the concept of three core functions:
- Assessment - Assessing needs of communities by collecting statistics and information related to the community's health needs. Assessment also means identifying the sources of health problems and the determinants of health and disease.
- Policy Development - Prioritizing public health needs, advocating for public health, building constituencies and coalitions and pursuing the enactment of policies and laws that promote health.
- Assurance - Establishing and maintaining an infrastructure for public health and implementing programs to monitor the effectiveness of public health interventions. Assurance also requires effective communication of public health information to the general public.
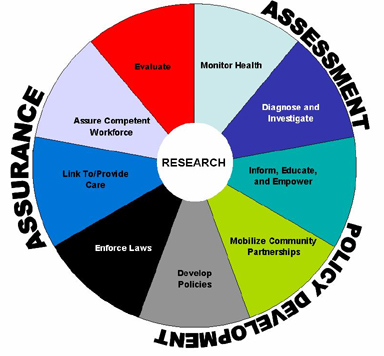
In 1994 the CDC expanded the 3 core functions and identified 10 essential services which should be undertaken in all communities, regardless of size:
- Monitor health status to identify and solve community health problems
- Diagnose and investigate health problems and health hazards in the community
- Inform, educate, and empower people about health issues
- Mobilize community partnerships and action to identify and solve health problems
- Develop policies and plans that support individual and community health efforts
- Enforce laws and regulations that protect health and ensure safety
- Link people to needed personal health services and assure the provision of health care when otherwise unavailable
- Assure competent public and personal health care workers
- Evaluate effectiveness, accessibility and quality of personal and population-based health services
- Research for new insights and innovative solutions to health problems
In 2002 the Institute of Medicine titled "Who Will Keep the Public Healthy?", which concluded public health professionals must have a framework for action and an understanding of the forces that impact health.
Population Health
The final decades of the 20th century placed heavy emphasis on individual responsibility for health and behavior modification. The newer definition by the CDC reflects a shift to population health. This shift was brought on by the recognition of the social determinants of health and acknowledgement of effective strategies to make communities safer and healthier. Other factors were threat of bio-terrorism, disparities in healthcare. During the 20th century, Winslow's definition of public health focused mainly on physical health of a geographical region, but this has been redefined in the 21st century to conciser mental health and envision populations not only geographically but by needs (the mentally ill, poor, those with HIV, etc).
Population health might include:
- Healthcare - Delivery of 1 on 1 screening, prevention, cure and rehabilitation
- Traditional public health - Surveillance, control of infection of disease and environmental hazards, food and drug safety, education to public, and behavior modification
- Social intervention - improvements to the environment, better access to healthy food, community safety and reduction in disparities.
Public Health 3.0
The birth and evolution of public health during the enlightenment is identified by the US Health and Human services separates into 3 eras: 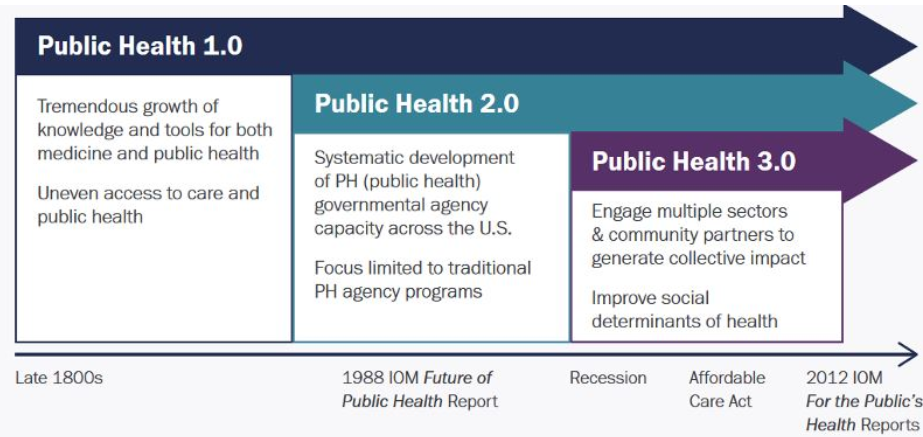
Public Health 1.0 - Modernized by the invention of vaccine, antibiotics, development of epidemiology, and advances in biological sciences. Led to advances in sanitation in safety.
Public Health 2.0 - Spurred by 1988 and 2002 report by National Institute of Medicine papers regarding the governments inability to act on mental health issues and HIV. The ability to cope with these problems were made worse during the budget cuts in the great recession (2008)
Public Health 3.0 - Innovative ideas on improving environmental factors in communities. Requires collective action and inter-organizational cooperation. In many communities the local health officer will take the role of Chief Health Strategist who guides community efforts and analyzes data mathematically to determine if best response has been enacted.
Health Impact in 5 Years
Achieving lasting impact on health outcomes requires a focus on community wide approaches to improve population health. Programs that address the conditions where we work and live. By changing the context that make healthy choices easier we can improve the health for everyone. The health impact in 5 years initiative highlights non-clinical community-wide approaches that have evidence reporting:
- Positive health impacts
- Results within 5 years
- Cost effectiveness or cost savings
The public health impact pyramid shows the potential impact of public health interventions. 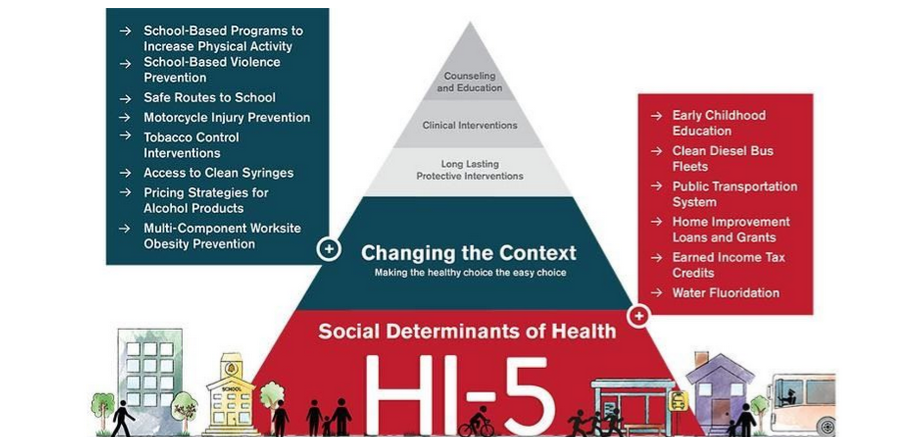 The base of the pyramid has the interventions that have the greatest potential for impact on public health. They reach entire populations at once and require less individual effort. The HI-5 initiative maps to the bottom 2 tiers of the pyramid with greatest potential which are often hardest to implement, and the most obvious aspect at the top.
The base of the pyramid has the interventions that have the greatest potential for impact on public health. They reach entire populations at once and require less individual effort. The HI-5 initiative maps to the bottom 2 tiers of the pyramid with greatest potential which are often hardest to implement, and the most obvious aspect at the top.
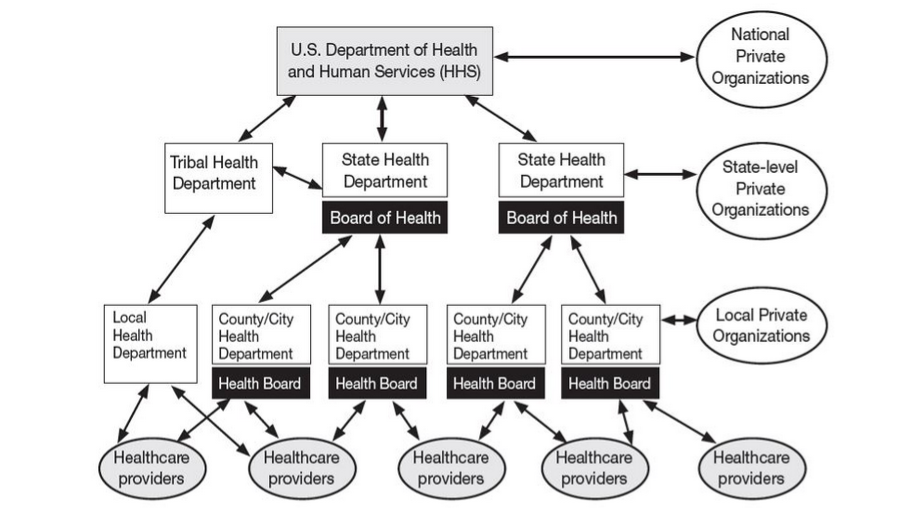
Public Health Structure
Unlike some countries, the US constitution does not explicitly establish a structure for provision of public health. However Congress has the power to levy funds to public health services. On a federal level, the US Department of Health and Human Services is responsible for protecting the health and well-being of all Americans by providing effective health and human services, and fostering advances in medicine and public health.
his Strategic Plan describes HHS's efforts within the context of five broad strategic goals:
Strategic Goal 1: Protect and Strengthen Equitable Access to High Quality and Affordable Healthcare
Strategic Goal 2: Safeguard and Improve National and Global Health Conditions and Outcomes
Strategic Goal 3: Strengthen Social Well-being, Equity, and Economic Resilience
Strategic Goal 4: Restore Trust and Accelerate Advancements in Science and Research for All
Strategic Goal 5: Advance Strategic Management to Build Trust, Transparency, and Accountability
Healthy People
Healthy people provides science-based 10-year national objectives for improving the health of all Americans. For 3 decades, Healthy People has established benchmarks and monitored process over time in order to:
- Encourage collaborations across communities and sectors
- Empower individuals toward making informed health decisions
- Measure the impact of prevention activities
Healthy People periodically sets 10 year agenda of goals for improving health in the US. Healthy People 2020 strives to:
- Identify nationwide health improvement priorities
- Increase public awareness and understanding of the determinants of health disease and disability and opportunity for progress
- Provide measurable objectives and goals that are applicable at the national, state, and local levels.
- Engage multiple sectors to take actions to strengthen policies and improve practices that are driven by the best available evidence and knowledge
- Identify critical research, evaluation and data collection needs
Police Power
Powers that are not specifically given to the federal government are retained by the states and referred to as police power. It allows each state to enact laws for the welfare to its citizens. Federal health laws supersede state laws, but in absence of federal law, states enact their own. Similarly, state laws take precedent over local laws. There is still significant interaction between HHS and state departments as well as national and state level organizations.
Philosophy and Ethics in Public Health
There are many definitions of public health, but the simplest is that public health is the constellation of actions that a society takes to enable people to enjoy good health and remain free of disease.
The goal of achieving a healthy society is intrinsically good, since it reduces disease, suffering and enables people to live longer, happier lives. These benefits have tangible benefits such as greater productivity and reduced spending on medical care.
While these goals are unarguably good, there is still debate as to how much money should be directed to public health when there is competition for limited resources, or whether the cost of a particular public health intervention justify the benefits.
Other considerations:
- What freedoms may be in conflict with the intervention?
- Do the benefits of interventions outweigh the potential for unknown risks?
Public health ethics involves the principals that guide us as a society in making decisions about public health that conform to our morals and standards while resolving or minimizing conflicts.
Learning Objectives:
- Discuss the philosophical justifications for public health
- Discuss the moral considerations for public health
- Discuss the justifications for overriding interests such as freedom of action privacy and confidentiality in order to achieve public health goals
- Explain the key questions that should be addressed when analyzing an ethical issue in public health
- Define the "police power" and discuss the major precedents set by Jacobson v. Massachusetts
Philosophical Justification
Several theories had significant impact on shaping public health ethics.
Jeremy Bentham was a proponent of utilitarianism, evaluating actions based on their consequences in producing happiness and contributing toward the greater good. His philosophy was "the greatest good for the greatest number".
John Stuart Mill was also a utilitarian but refined his views to distinguish higher and lower pleasures. "The only purpose for which power can be rightfully exercised over any member of a civilized community, against his will, is to prevent harm to others." He was not absolute on this, as he acknowledged that no system of ethics requires the sole motive of all we do be based on duty. 99% of all our actions are done from other motives, and rightfully so if the rule of duty does not condemn them.
"Public Health draws its foundational legitimacy from the essential and direct role that health plays in human flourishing... However, the general justification is sometimes too broad to provide sufficient moral warrant for specific public health policies which are implemented by the state and affect the liberty or privacy or corporate or individual persons." -JSM
Overall Benefit
All individual population members benefit from public health agencies and interventions, even if they don't benefit from all interventions. Agencies such as the CDC and FDA are charged with improving health within the population. While public health regulations may pose restrictions and inconvenience to some of us, the overall effect is an improvement in the quality of our lives.
Collective Action and Efficiency
Public health operates at the population level, and many of its benefits could not be achieved without regulation and coordinated efforts of many trained people with special expertise. For example, food safety at the level we currently enjoy could not be achieved without extensive, coordinated effort by many agencies.
Fairness in the Distributions of Burdens
A basic premise is that burdens and benefits should be distributed fairly. For example the requirement for childhood vaccinations encourage high levels of population immunity and provides a distribution of both the benefit of protection and the burden of having to get vaccinations.
The Harm Principal
John Stuart Mill established what we now know as the harm principal, which states power can be exercised over members of a society when the purpose is to prevent harm to others. This principle provides justification for limiting individual freedom through isolation or quarantine to control the spread of disease, and even for mandatory treatment in some instances.
This was also an important justification for banning smoking in public places once there was evidence of harm from secondhand smoke. This brings up the question regarding the extent of harm and weighing in on the curtailment of personal liberty. Mill recognized by separating lesser freedoms and fundamental freedoms that should not be interfered with in the absence of compelling justifications.
Paternalism
Paternalism generally has a negative connotation implying unwanted interference. However, the notion of paternalism as a justifications comes into play in the context of protecting vulnerable people such as those with cognitive disability or immaturity (situations where autonomy is already compromised and protection is needed).
Moral Considerations
The United States, constitution recognizes that police power is needed to enforce laws to promote health, safety and general welfare. This led to the concept of "strict scrutiny" whenever the use of police power threatens fundamental freedoms. Ex:
- Is there justification for the state to require citizens to use seat belts while driving or helmets while riding a bike?
- Is there justification for quarantining citizens with active tuberculosis to ensure they take their medications?
Ethical essentials of public health:
- Producing benefits
- Avoiding, preventing and removing harms
- Distributive justice - distributing benefits and burdens fairly - and procedural justice - meaning ensuring public participation
- Autonomy - respect for autonomous choices and actions
- Protecting privacy and confidentiality
- Keeping promises and commitments\
- Transparency - disclosing information honestly
- Building and maintaining trust
Justification for Infringing Interests
Effectiveness
One important question is whether there is reason to believe that a proposed public health intervention, such as quarantine, would be effective. If not, it would not be ethically justified to restrict individual liberty.
Necessity
Even if forced quarantine might be effective, it might not be necessary. For example, Tuberculosis (TB) is one of the great killers of all time, especially in recent years due to the emergence of a multiple-drug resistant TB. The CDC recommends Directly Observed Therapy (DOT) in which the patient is required to meet with a health care worker every day or several times a day to ensure the medications are taken. New York City uses a tiered system of DOT. Most patients are observed taking their medications via smart phone. However the city may impose quarantine on TB patients at Bellevue Hospital, but these extreme measures are only used in extreme measures when infectious people habitually fail to take their medication. Every alternative must be exhausted before infringing on personal liberties.
Least Infringement of Presumptive Value
In any given circumstance the least restrictive infringement that enables the goals to be achieved is the one that should be utilized. NYC's tiered DOT system is a good example. Similarly, if it were justifiable to breach privacy or confidentiality, the breach should limit the information disclosed as much as possible.
Proportionality
Even after satisfying the previous three justifications, one must also consider whether the likely benefits justify the cost, both financially and in terms of personal interest. Here is a list of interventions from the most restrictive to the least restrictive:
- Eliminate choice
- Restrict choice
- Guide choice by incentives
- Guide choice by changing the default policy
- Enable choice
- Provide information
- Do nothing
Impartiality
There have been a number of instances when coercive measures such as quarantine were applied more rigorous to certain categories of citizens. For example, coercive measures were applied disproportionately against the Chinese during the SARS outbreak in 2003.
Involvement of the public in deliberations about public health is essential, since community members are the most important stakeholders. Public health activities and interventions should be carefully explained to community members honestly and transparently.
Analyzing Ethical Issues
There are several key questions public health policymakers should address when analyzing ethical issues:
- What public health problems, needs, or concerns are at issue?
- What are appropriate public health goals in this context?
- What is the source and scope of legal authority, if any, and which laws and regulations are relevant?
- What are the relevant norms and claims of stakeholders in the situation and how strong or weighty are they?
- Are there relevant precedent legal and ethical cases?
- Which features of the social-cultural-historical context are relevant?
- Do professional codes of conducts provide guidance?
Public Health Law
Jacobson V. Massachusetts
In 1900 smallpox was still a significant issue. In 1900 there were 100 cases of smallpox in MA. By 1902 there were over 2300 infections. The board of health became concerned and mandated all citizens should get a smallpox vaccine if they had not been vaccinated since 1897. It was within the board's power to do so and had already been proven that vaccines were an effective measure for prevention. Many citizens were opposed to vaccines for various religious, political, and philosophical arguments as well as concerns about safety. Jacobson was a Swedish Reverend in MA who refused vaccination and was fined $5. He sued, and lower courts upheld the fine and eventually it went to the SCOTUS where the court ruled in favor of the state. In essence, their decision ruled that public health laws have to be rational and reasonable noting that there are times we must give up our personal liberties for the common good. This case has been used as precedent on many following lawsuits, such as those regarding quarantine or mandating helmets on motorcycles.
Police Power
While the power to create public health law exists in all levels of government. One could argue most the power of public health authority lies at the state and local level where police powers exist, the ability to enforce policy to help guide the health and welfare of the citizens. The 10th amendment of the Bill of Rights specifically reserves police power to the states and sometimes local authorities. The federal government can collect funds from taxes and distribute them to programs, or regulate commerce to stop the spread of disease. State and local health departments are responsible for the public health of their communities, rather than the CDC.
Legal Epidemiology refers to the study of law as a factor in the cause, distribution, and prevention of disease and injury. It applies rigorous, scientific methods to translate complex legal language into data that can be used to evaluate how laws affect population health. The idea that law is a major determinant of health is only just starting to evolve, we are still studying the most effective interventions on smaller populations before introducing it to a larger population.
Principals for Public Health Professionals
In 2010 a CDC sponsored project published a code of ethics for public health. Public health should:
- Address principally the fundamental causes of disease and requirements for health, aiming to prevent adverse health outcomes
- Achieve community health in a way that respects the rights of individuals in a community
- Develop policies programs and priorities that are evaluated through processes that ensure an opportunity for input from community members
- Advocate for, or work for the empowerment of, disenfranchised community members, ensuring that the basic resources and conditions necessary for health are accessible to all people in the community
- Seek the information needed to implement effective policies and programs that protect and promote health
- Provide communities with the information they have that is needed for decisions on policies or programs and should obtain the community's consent for their implementation
- Act on a timely manner on the information they have within the resources and the mandate given to them by the public
- Incorporate a variety of approaches to programs and policies that anticipate and respect diverse values, beliefs, and cultures in the community
- Be implemented in a manner that most enhances the physical and social environment
- Protect the confidentiality of information that can bring harm to an individual or community if made public. Exceptions must be justified on the basis of the high likelihood of significant harm to the individual or others.
- Ensure the professional competence of their employees
- Engage in collaborations and affiliations in ways that build the public's trust and the institution's effectiveness
Evidence-Based Public Health
Maximizing the health of a population is largely achieved through three core functions of public health; Assessment, policy development, and assurance. Within each core function lies a subset of the 10 essential functions of public health:
As mentioned in the the previous module on ethics, it is essential to consider alternative courses of action to maximize benefit, minimize adverse consequences and make the most efficient use of scarce resources. As a result decisions on how to address public health must be evidence-based, meaning they are based on accurate and complete data which have been rigorously analyzed.
Two broad types of evidence are essential to the practice of public health:
- The Evidence regarding the efficacy and adverse consequences of interventions
- Evidence regarding the determinants of health and disease
In addition, it is useful to have evidence regarding how a disease spreads across a population, including social and political factors. Ex. are there members of the population at higher risk due to behavior, age, preexisting conditions or geography?
Even though most research depends on quantitative data, a fine understanding usually requires qualitative data.
Learning Objectives:
- Describe the general steps involved in identifying and addressing public health problems
- Describe and give examples of the role of surveillance systems in public health
- Explain what is meant by the term "notifiable/reportable disease"
- Describe the breadth of modern public health surveillance systems and give specific examples
- Define "syndromic surveillance" and explain how it can be advantageous over regular surveillance
- Explain how the characteristics of person, place, and time are used to formulate hypotheses in acute disease outbreaks and in studies of chronic diseases
- Distinguish among case reports, case series, cross-sectional surveys, and ecological studies and explain their importance
- Explain the concept of ecologic fallacy
- Describe the difference between descriptive and analytic epidemiologic studies
- Define and explain the distinguish between retrospective and retrospective cohort studies
- Define and explain features of a case-control study
- Explain and distinguish features of of an intervention study (clinical trial)
- List and define 3 major threats to validity in analytical studies
- Describe the contribution of quantitative and qualitative research to public health
Four Steps
Rothman summarized the four steps to public health approach as followed:
1. Identifying the Problem
In the US there are number of ways in which public health problems are identified:
- Surveillance systems monitor and record occurrences of specific infectious diseases, and information is communicated from municipalities or counties to state health departments and then federal agencies
- States maintain cancer registries
- Computerized registries are increasingly used for diseases like diabetes, kidney failure, and a variety of other problems
- Vital statistics regarding births, deaths, marriages, and divorces are collected by each state and other jurisdictions and through co-op agreements that data is shared with the US National Vital Statistics System
- Many federal agencies periodically conduct surveys to monitor health status of the population
- Health care providers report new or unusual problems to health departments and disseminate findings in the form of case reports or case series
- Local and federal organizations and systems are in place to inspect food and monitor water quality
2. Identifying Contributory Causes
Epidemiology is a discipline that studies the distribution of health outcomes and its possible determinants in populations in order to identify casual associations. Epidemiology us described as the basic science of public health, because it is based in scientific method and identifies factors associated with health states by systematically collecting, analyzing and interpreting quantitative data.
3. Identifying What Works
This is also largely achieved through quantitative methods that evaluate the efficacy of interventions through clinical trials and program evaluation.
4. Identifying the Means
This may rely on quantitative methods, but increasingly relies on qualitative research which aims at understanding people's perceptions and developing an understanding of why they believe what they do. Ex interviewing a key informant to see why a particular intervention did or did not work in order to improve future programs.
Surveillance Systems
Surveillance for public health is based on a variety of data sources that track health status and health-related behaviors in a population over time in order to identify new problems, such as infectious disease outbreaks. In addition to monitoring trends these data help identify new health problems and provide clues about the causes of new issues in a population. Surveillance data enables us to:
- Monitor and report on the health status and health related behaviors in a population
- Identify emerging health problems
- Alert us to potential threats
- Establish public health priorities for a population
- Evaluate the effectiveness of intervention programs
- Explore potential associations between risk factors and health outcomes in order to generate hypotheses about the determinants of disease
Passive Surveillance
Routine reporting of health data. Can create a full picture when combined but is limited by under-reporting.
- Hospital Data
- Disease registries
- Notifiable diseases - Some countries have laws which list diseases which are required to report
Active Surveillance
Actively sought out information:
- Active case finding
- Testing blood markers
- Community Surveys
Sentinel Surveillance
A group of selected institutions or groups pool health data together on a certain disease. This can be used to monitor disease outbreaks and trends, but is unable to detect cases outside sites/groups making it ineffective for rare diseases.
Rumor Surveillance
Relies on unofficial sources of information (blogs, social media, hearsay, etc.). It might alert authorities to investigate further for signs of an outbreak.
Syndromic Surveillance
Monitors for non-specific illness syndromes recorded at medical clinics, along with tells like medicine purchases or absenteeism from school or work. Allows for early identification and can rely on automatic reporting methods. A "syndrome" is a cluster of signs and symptoms.
Other Types
- ProMED - Web-based
- GPHIN - Early warning tool to monitor significant health events
Characteristics of a Good Surveillance System (from CDC)
- An integrative approach uses all available information and provides the best overall picture of health
- It has simple, clearly defined objectives
- The data should be complete and accurate
- The plan should be flexible without incurring additional costs
- Accepted by people and organizations involved in public health surveillance
- Sensitive and Positive Predictive Value (PPV), it should pick up most if not all cases of the disease in the population
- It accurately measures what it intends to measure
- Timeliness to leave room for action
- Stable and available when needed
And all surveillance systems should be evaluated on their effectiveness and if they meet public health functions
Data Sources
There are many sources of data that are useful for monitoring health of the populations and exploring disease frequency over time. Ex:
- Census and Records - US Census and US National Vital Statistics System and the Massachusetts Registry of Vital Statistics and Records
- Disease registries - Massachusetts Cancer Registry, ALS Registry
- Hospital Discharge Registries
- Community Health Information - In MA the Community Health Information Profile (MassCHIP) provides a dynamic, user-friendly service for obtaining free online access to many health and social indicators. One can obtain community-level data to assess health needs, monitor health status indicators and evaluate health programs.
- Infectious Disease Surveillance - Division of Emerging Infections and Surveillance Services (DEISS)
- Commercial Data - Sale of tobacco, drugs, etc
Reportable Diseases
Each US state designates a specified list of diseases that are required to report by law. The MA Department of Public Health provides a Reportable Diseases web site as an online resource for all public health organizations. This data is fed into the National Notifiable Disease Surveillance System (NNDSS).
Data for selected nationally notifiable diseases reported by the 50 states and D.C. and the US territories are collated and published weekly in the Morbidity and Mortality Weekly Report (MMWR).
Descriptive Epidemiology
Descriptive epidemiology is defined as epidemiological studies and activities with descriptive components that are much stronger than their analytic components or that fall within the descriptive area of the descriptive-analytic spectrum.
When new health problems arise, health practitioners need to find details on the determinants. The most basic starting point is to collect detailed information about a single case (case-report) and search for additional persons with similar cases and gather information from a series of similar cases (case series). The most fundamental information focuses on three key aspects: Person, place, and time. These fundamental elements enable us to look for suggestive patterns.
- Person - all relevant characteristics including age, diet, behaviors, exposures, etc.
- Place - Spatial distribution of the problem.
- Time - Whether the frequency of disease varies over time.
- Differences - Factors may cause the frequency of disease to differ in circumstances
- Similarities - A high frequency of disease found in several different circumstances with a common factor
- Correlations - If the frequency of disease varies in relation to some factor
Epidemiological Studies
A study is a scientific process of answering a question using data from a population. The first step is having a question to study, then decide a study type, collect and analyze data (ethically), interpret results, and reporting findings.
Types of studies
Ecological Study
Disease rates and information about exposures are made on a group of people. Could be a household or an entire country. Results apply to groups and not individuals, meaning these studies are better at comparing health between populations and generating questions.
Case Series
Describes characteristics of people with the same disease or exposure.
Cross-Sectional/Prevalence Study
Health information of a selected population at a given point in time. Usually involves a questionnaire or survey and are relatively inexpensive, but it cannot determine if exposure caused a disease because the data is collected from a single point in time (i.e. which came first) and also tend to favor cases with a longer duration and overlook cases which recovered quickly.
Case Control Study
People with a disease, called cased, and people without the disease but with similar characteristics, called control, are asked about past exposures to certain risk factors. For each risk factor the odds of being exposed as a case is compared to the odds of being exposed if they were control, giving us the Odds Ratio (OR).
| Cases (Have Disease) |
Controls (No Disease) |
|
| Exposed |
a |
b |
| Unexposed |
c |
d |
Odds Ratio (OR) = (a/c) / (b/d) = a*d / b*c = Odds that a Case was Exposed / Odds that a Control was Exposed
Relative Risk (RR) = (a / (a + b)) / (c / (c + d)) = Risk of Disease of Exposed / Risk of Disease Unexposed
If the OR is greater than 1 than the risk factor is associated with disease, less than 1 suggests its a protective factor and =1 suggests no association.
This is often used when searching for food-borne illnesses. They are quick and cheap, and can be used for uncommon disease. It falls short when finding rare exposures, and it can be difficult to find a representative control selection who can accurately recall if they were exposed.
Cohort Study
A group of people are followed over a period of time to collect data on risk factors and then compare occurrences of similar outcomes of those who were exposed and those who were not.
The main measurement used in cohort studies is called the Relative Risk (RR), which is the risk of disease for those exposed to a risk factor over the risk of disease in the unexposed group.
RR > 1 is increased risk, RR < 1 is lower risk, RR = 1 is same risk
Advantages are that time sequence can be determine causality and info on various outcomes/risk factors can be collected at the same time. Disadvantages are the fact that many people have to be followed over a long period of time make them costly and not good for rare diseases, also if too many people drop out it will interfere with the results of the study.
Interventional Study
Intervention is done on a group and outcomes are measured. This could be medicine, vaccine, health advise, etc.
The best design for an interventional study is a randomized controlled trial, where people are randomly selected from the population to either receive the intervention or take part in the control group. Ideally the experiment would be double blind, where neither the participant or investigator know who is the control group.
These studies can provide good evidence of causality, and randomization provides equal chance that groups are similar. Disadvantages are the cost of finding participants.
Summaries
Summaries are studies made with other studies. Systematic review finds all relevant studies to a topic, assesses and interprets the results and creates an unbiased, impartial summary of the evidence. A meta-analysis uses data from studies which asked the same question and had a similar design, then uses that data to combine analysis and produce a single summary result.
Examples of Descriptive Epidemiology
Case Report
A detailed description of disease occurrence in a single person.
Ex. April 1983, it was not yet know AIDS could be transmitted by blood. An infant born with a blood disorder required transfusion from 18 donors over 8 weeks and later developed a low T cell count suggesting AIDS. It was later found one of the donors died of AIDS.
Case Series
A report on the characteristics of a group of subjects who all have a particular disease or condition. Cannot be used to infer causality because there is no comparison group, but can be used to hypothesize questions for a study.
Ex. 1981 Pneumonia study on previously healthy young men, which was an important milestone in the AIDS epidemic. Case studies cannot establish a valid association but in this case laid the groundwork for subsequent case-control and cohort studies.
Cross Sectional Surveys
Surveys which assess the prevalence of disease and risk factors at the same point in time.
Ex. US government agencies sent surveys to random samples of the US population asking about health status and behaviors. There was a heart disease survey given to farmers asking only if they were physically activity. Because the participants were not followed, we can't tell if the cases developed heart disease because they were inactive, or if they are inactive because they developed heart disease.
However, in some circumstances the temporal relationship is clear. Ex. a study which measures salary between male and female employees could be regarded as analytical because gender was already established because the outcome (salary). In a sense, cross sectional and ecological studies are an intermediate category between descriptive and analytic studies.
Ecological Studies
These studies are distinguished by the fact the unit of observation is not a person but an entire population.
Ex. Comparing the rate of colon cancer based on meat consumption in different countries. The issue is the study assumes everyone in each country has the same exposure, or ate the same amount of meat. There is no information about individual people, thus there is no way of knowing if the people who ate the most meat are the ones who developed colon cancer. This is referred to as ecological bias or ecological fallacy.
Analytical Studies
Descriptive epidemiology is useful for generating hypotheses about determinants of health, but they have a number of limitations that do not allow them to firmly establish a valid association between a given factor and a health outcome.Analytic studies are more formal comparisons that enable investigators to test specific hypotheses. Samples of subjects are identified and information about exposure status and outcome is collected and analyzed in order to estimate the magnitude of association.
Prospective Cohort Studies
A cohort is an identified individual who does not have the outcome of interest initially, but have potential to develop the outcome of interest.
Ex. Framingham Heart Study enrolled residents who did not have cardiovascular disease when enrolled and followed them to see if and when they developed cardiovascular issues.
Retrospective Cohort Studies
In contrast to prospective cohort studies, retrospective cohort studies are conceived after some subjects have already developed the outcome of interest. Investigators jump back in time to identify a cohort of individuals at a point in time before they developed an outcome and try to establish exposure.
Ex. studying employee health records at a chemical plant after multiple employees die. The preexisting data was data may not be acquired in a predetermined way or may be incomplete.
Intervention Studies
Experimental research studies that compare the effectiveness of public health interventions or medical treatments. The design is similar to prospective cohort studies, except that the exposure is assigned by investigators. Exposure status is assigned randomly to produce equal effects of confounding variables.
Ex. A drug treatment trial with a placebo group.
Case Control Studies
Cohort studies fall short when the outcome being investigated is rare, or there is a long period of time between exposure and outcome. In a case control study, investigators start by finding an adequate number of cases who already have the outcome and a comparison group without the outcome and all are sorted into an exposed or unexposed categories.
Rare Disease in Plymouth County
In this hypothetical situation Plymouth County has a total population of 6647.
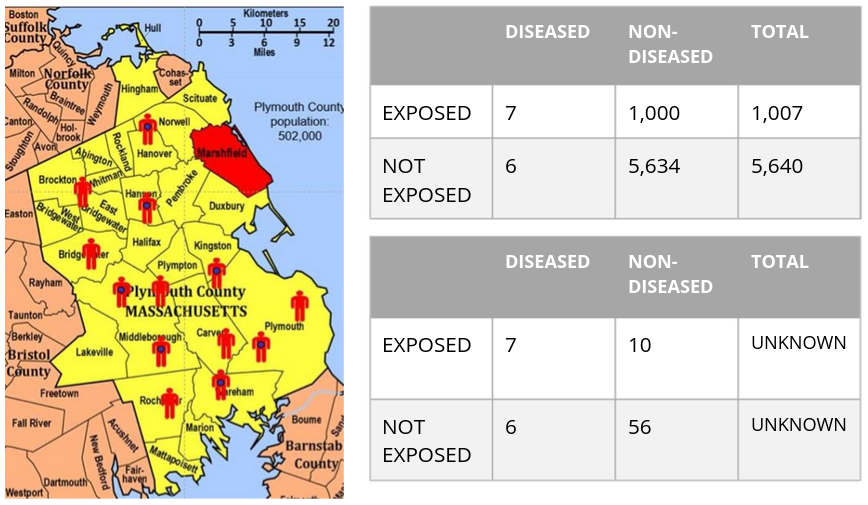
If we somehow had all the exposure and outcome information in the source population we could calculate the incidence of exposed and non-exposed individuals and calculate the risk ratio.
Ie = 7 / (1000 + 7) = .70%
Iu = 6 / (6 + 5634) = .11%
RR = .7 / .11 = 6.5
Meaning those exposure to the risk factor had 6.5 times the risk of getting the disease.
However, in practice we rarely have the resources to get data on all subjects in a population. In the lower table we take a sample of 1% of the non-diseased population. We can't predict the Risk Ratio because we don't know the denominator, but we can compute the odds of disease in each group
Oe = 7:10
Ou = 6:56
Odds Ratio = (7/10) / (6/56) = 6.65
This is very close to the risk ratio and thus is a reasonable estimate.
Which Study is best?
- If the outcome is uncommon a case control study would be best
- If the exposure is uncommon a cohort study is best
- Consider ethics: if studying the association between smoking and cancer it wouldn't be ethical to conduct a clinical trial in which you randomly assign half the subject to smoking
- Resources: If you have limited time, money and personnel to gather data it is unlikely that you will can conduct a prospective cohort study. A case-control study or retrospective cohort study would be better options, depending on if the outcome or exposure was more rare
Sources of Error
Random error (Sampling Error) - Samples may provide estimates of relationships in the population that are inaccurate, particularly if the population size is small
Bias - Estimates of parameters in the population may be distorted by errors in the data collection (information bias) and if the selection or retention of subjects into our samples is somehow dependent on the exposure-outcome relationship (selection bias)
Confounding - a particular type of bias that occurs when other determinants of the outcome are unevenly distributed in the groups being compared
Program Evaluations
To know if programs and interventions are effective one needs to answer several critical questions:
1. Is the program meeting its objectives? Why or why not?
2. What are the strengths of the program?
3. How might the program be improved?
4. What can be learned from current or past programs to improve future programs?
Types of Program Evaluation
Formative
The goal is to obtain feedback on strengths and areas of improvement for the program and explore overall applicability and feasibility of the project. Typically takes place early in the inception to determine whether the program is applicable or makes sense.
Ex. Focus groups at a community center, pen and paper surveys, one-on-one interviews with members of the target community
Process
Addresses whether the program was implemented as intended and why it did or did not meet its main objectives.
Ex. Access what percent of a online education model was completed, interview program coordinators
Outcome/Impact
Measure the overall effectiveness of the program in meeting its objective.
Ex. Observing teen pregnancy rates 5 years after a sex education course.
Framework for Program Evaluation
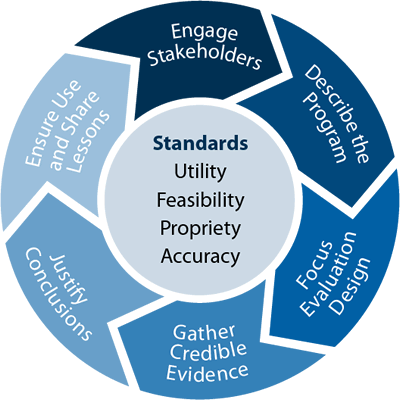
Engage Stakeholders
An accurate, valid evaluation is a major goal for evaluators, but ultimately the strongest evaluation is the one used to beget action. In order to do so, a critical step is to consider the evaluation audience (stakeholders) and who is most invested.
Describe the Program
Elucidate and explore the program's theory of cause and effect, outline and agree upon program objectives, and create focused and measurable evaluation questions.
Focus Evaluation Design
Consider your hypothesis and available resources and weigh different design options to understand advantages and limitations of design options.
Gather Credible Evidence
Data collection is essential to support evaluation conclusions and recommendations. What you collect and how directly impacts the quality and credibility of findings.
Justify Conclusions
Use the evidence and data analysis to answer the main research questions and create conclusions and recommendations.
Use and Share Lesson Learned
The primary goal of an evaluation should be useful and this requires communicating and sharing results. Stakeholders should be aware of the study process, findings, and efforts should be made to ensure results are incorporated into program decisions.
Qualitative Reseach
Quantitative research are designed to precisely measure the association between biological, social, environmental, and behavioral factors and health conditions.
Qualitative research methods focus on understanding why and how individual life experience and the context of community life influence health and wellness. Such contextual information is difficult to capture through traditional quantitative surveys. Methods that rely on rapport and trust between researcher and participant that include open-ended questions enable participants to talk about their perceptions and experiences Qualitative methods may be employed in combination with quantitative methods during the research process.
Mixed Methods Research
When qualitative and quantitative methods are blended in the context of a research study, we refer to it as a "mixed methods research." In such cases it is common to employ qualitative methods to:
- Generate hypotheses which may be applied to intervention design and evaluation
- Enrich Understanding about a research topic that may be inaccessible using quantitative methods
- Provide insights that specialists and researchers may not considered beforehand
- Facilitate partnership between researcher and community members affected by the heath issue under study
Comparison of Research Methods
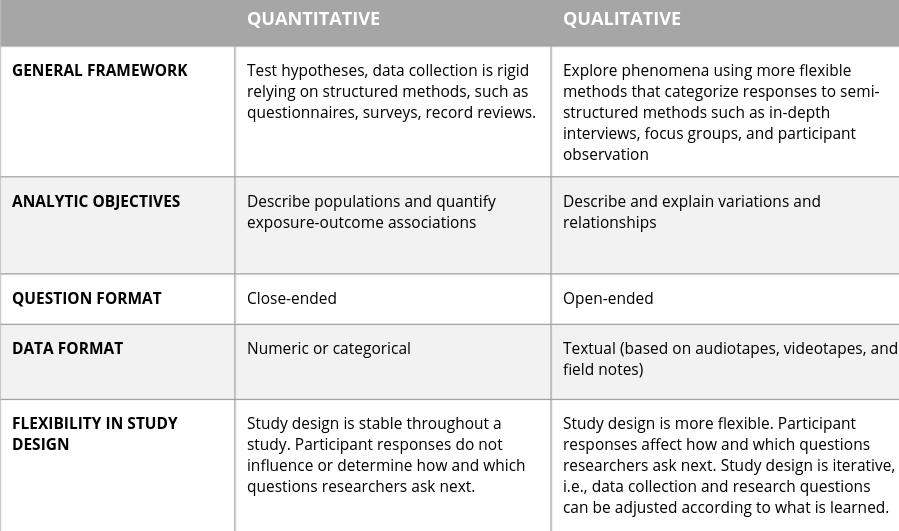
The product of qualitative research can be recurrent themes or hypotheses by identifying salient factors and informing predictions about relationships. Themes are unifying concepts that identify and characterize a pattern of behaviors, group interactions, or individual perceptions.
Learning Objectives
- Articulate the purpose and significance of qualitative research methods
- Determine when it is appropriate to use qualitative methods to address research
- Illustrate ethical considerations in the conduct of qualitative methods
- Define the major qualitative research techniques, their strengths and limitations and contexts in which they are best used
- Define and illustrate the importance of "Community-based Participatory Research" (CBPR) as a research design often involving qualitative methods
Common Qualitative Methods
Participant Observation
Collecting data on behaviors in natural settings; study cultural aspects of a particular setting. Usually conducted early in a study but can be used to follow up as well. The role of the participant/observer is to careful observe all details with a wide angle lens.
- Non-participation: No involvement with the people or activities studied (ex. studying television programs)
- Passive Participation: Present at the scene where activities take place, but does not participate in them or interact with other people. (Ex. Court or clinic waiting room observer)
- Moderate Participation: Balance between insider and outsider / participant and observer. (Ex. Participating in a town meeting)
- Active Participation: Active involvement in what your subjects are doing. (taking a minimum wage job to see how poor people manage expenses)
- Complete Participation: Some who is already involved in a particular activity or part of a particular group to specifically record systematic observations.
In-Depth Interviews
These are the best way of collecting in-depth information on personal histories, opinions, and life experiences. These can be unstructured, semi-structured, or structured interviews. The idea is to have a guided discussion reflecting the individual's perspectives and experiences. The researcher might read questions from a prewritten guide which are open-ended in order to have the participant lead the discussion. These are great for sensitive topics when surveys or focus groups are ineffective.
Focus Group Discussion (FGD)
These provide a means of collecting data on cultural perspectives and norms of a group. Usually about 5-10 people, with 3-5 groups per strata, discussing a set of predetermined topics. Stratification is the breakdown of groups based on how similar or different members of the group should be. These strata could be characteristics such as age, wealth, race, etc. These are useful for characterizing social and cultural norms or exploring how people talk about a sensitive topic. Keep discussion open-ended and avoid asking why or for examples. The group is the unit of analysis, not the individuals within it.
Community-Based Participatory Research (CBPR)
Over the past 25 years it has become increasingly apparent that there is a health disparity in people living in disadvantaged communities, which is why it is crucial to move beyond traditional approaches which have previously led to breaches of trust and deep divides between researches and the community.
Minkler and Wallerstein state: "CBPR begins with an issue of real importance to the community and involves the stakeholders and community members throughout the research process, including its culmination in education and action for social change." CBPR is not a method but an orientation; subjects are not objects of research but active participants. It's like a potluck with everyone bringing knowledge and expertise to the table. Note there are several names given to such approaches.

CBPR can...
... support the development of research questions that reflect issues of real concern
... improve our ability to achieve informed consent and address "cost and benefits" at the community level
... improve cultural sensitivity and reliability and validity of measurement tools
... uncover knowledge critical to enhancing understanding sensitive health issues
... improve recruitment and retention efforts by increasing community trust
... increase the relevance of intervention studies, and thus the likelihood of success
Qualitative Data Analysis
Qualitative data analysis is the process of organizing, coding and examining raw data and finding patterns in order to interpret or understand behavior and social phenomena.
Data could be in the form of texts, audio-recordings, images, and artifacts. Software programs such as NVivo are useful for managing qualitative data. In such programs the analyst does the coding of the data himself, which allows them to identify major themes. There are two type of coding; Inductive, which is often done at the formative stage of research and relies on "open" coding to allow meaning to emerge from the data, and deductive, which is usually done at the confirmatory stage and starts with a hypothesis before starting to code.
Using a qualitative research approach means:
Criticisms of Qualitative Research
- Lacks reproductability
- Lacks generalizability
- Researcher bias
Qualitative Articles Should Report:
- Relevance of question and rational for approach
- Sampling strategy (selection, saturation)
- Data collection (interview guide, depth of data)
- Analysis (number of coders, training, code structure, systematic process, software, divergent cases, participant confirmation, audit trail)
Trends in Morbidity, Mortality and Behaviors in the US
To follow trends in the causes of disease and death, the two measure of incidence that are always of interest are mortality and morbidity rates.
Mortality Rate: The incidence of fatal cases of a disease in a population during a specific time period.
Morbidity Rate: The Incidence of non-fatal cases of a disease in a population during a specific time period.
Learning Objectives
- Define and calculate mortality and morbidity rates
- Identify major causes of mortality and morbidity
- Discuss gender and racial differences in overall mortality trends
- Discuss trends in the major causes of mortality and morbidity
- Discuss the temporal relationship among per capita cigarette consumption
- Discuss where the US ranks among nations in regard to infant mortality rates
Trends in Mortality
In order to adjust for differences in age distribution of the population over time researchers computed age-adjusted death rates per 100,000 population per year, finding that from 1969 to 2013 mortality rates decreased by almost 50%. Mortality rates in males were greater than females across the entire period.
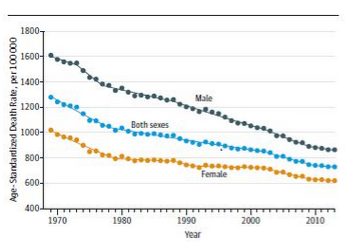
One size does not fit all in the US. A breakdown of reasons for death revealed a variety of trends in different parts of the country. I.e. violence related deaths are more common on the West Coast, while heart disease related deaths are increasingly common in the Southeast. While death by heart diseases are slowly declining overall due to declining smoking rates, while in comparison the rate of COPD has been increasing since the 80's. This is because it takes many years for COPD to manifest. Heart disease is still the leading cause of death in US.
Years of Potential Life Lost (YPLL) is an estimate of the average number of years a person would have lived had they not died prematurely, it is a measure of premature mortality. To calculate YPLL one must establish a reference age for the population.
Biological Foundations for Public Health
An overview of the understanding of the biological basis to health problems
Infectious Agents
Learning Objectives
- Explain the major differences between prokaryotic and eukaryotic cells
- List major types of infectious agents and be able to distinguish between living and non-living
- Explain key differences among bacteria, fungi, protozoa, and prions
- Describe how bacteria and viruses reproduce
- List and describe the four general patterns of viral infection
- Define 'prion' and discuss the role of prions in the epidemic of bovine spongiform encephalopathy (BSE) in the UK
- Discuss the role of prions in Creutzfeldt-Jakob Disease (CJD)
- Discuss how the British BSE epidemic in cattle caused disease in humans
The 5 Kingdoms
Every species can be categorized as a plant, animal, bacteria, fungi, or protozoa. While natural selection implies competition among and within species there is a strong interdependence among species. For example, most bacteria are non-pathogenic and live in and outside our bodies and provide many benefits, such as preventing pathogenic species from gaining a foothold.
Bacteria
Healthy internal tissues are free of microorganisms but skin & mucus membranes in our gastrointestinal tract, respiratory tract, and genito-urinary tract are in contact with organisms in the environment and become colonized with many bacterial species. These bacteria are referred to as "normal flora". The normal flora for a human consists of more than 200 species of bacteria, which depend on a variety of factors.
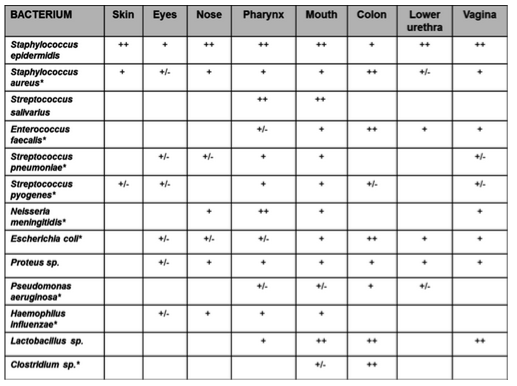
The above chart shows several common bacterium and where they are commonly found on the human body. (+/--) denotes they may or may not be present (++) means they are most always.
These normal flora provide a variety of benifits which include:
- Prevent colonization by pathogens by competing for attachments & netrients
- Some synthesize vitamins that are absorbed as nutrients by the host (e.g. K & B12)
- Some produce substances that inhibit pathogenic species
- Simulate production of cross reactive antibodies. Since normal flora behave as antigens in an animal, they induce low levels of antibodies that cross react with similar antigens on pathogens, preventing infection
- With the help of fungi, bacteria play a vital role in breaking down dead organisms
Some data suggests the inappropriate use of antibiotics and avoidance of microbes through disinfecting ourselves and our environment may have adverse effects on health. Over-disinfection in children may increase risk of autoimmune disease, obesity and asthma.
Bacteria as Pathogens
While only 5% of bacterial species are pathogenic, bacteria have historically been the cause of a disproportionate amount of human disease and death. Among those born in the UK in the 1800s, it is estimated that 70% died before the age of 25 and a large proportion of deaths were due to bacterial infections. Unsurpisingly, the burden of disease then still fell most heavily on the poor. However, during the 19th century the emergence of "the sanitary idea" in the UK and US made efforts to provide better water, waste disposal, nutrition, and all around better working conditions that was rewarded with a remarkable reduction in disease and death rate.
Prokaryotes Vs Eukaryotes
The bacteria are the oldest and simplest living organisms and all of the bacteria are "prokaryotes" meaning they do not have a true membrane-bound nucleus as eukaryotes do.
Prokaryotes
- Simpler than eukaryote cells
- Have a cell membrane and cell wall, and may have a gummy exterior capsule that enables bacteria to attach to surfaces and resit drying out
- May have a pili; a pilus is a hairlike projection from the cell membrane that aids in attachment
- May have a special sex pilus which forms a tube like bridge between two prokaryotes to enable transfer of plasmids (extrachomosomal genes)
- Tend to have a single chromosome composed of DNA, sometimes referred to as "nucleoid" because there is no nuclear membrane surrounding it. There are also ribosomes that are free-floating within the cytoplasm.
- May have simple whip-like flagella that enables them to be motile in fluid environment
Fungi
- Fungi are plant-like are were once classified as plants, but lack chlorophyll and differ in other ways so are now classified in a separate kingdom
- Fungi are structurally different from plants, and are not truly multi-cellular
- Fungi are sometimes mutualistic, living with other species and growing with symbiotic relationship on rocks & trees.
- They can provide food, nutrients and yeasts enable the fermentation of sugar to alcohol
- Sometimes they provide a source of antibiotics, in 1928 Sir Alexander Fleming observed colonies of bacterium could be destroyed from the mold pennicillum notatum
- Fungi are saprophytes that decompose dead organic matter by growing into a substrate and absorbing nutrients from it
- Parasitic fungi often feed on living organisms without killing them (e.g. ringworm & athletes foot)
- Fungi are generally composed of branching filaments (hyphae) that sometimes form a large interlacing mass called a "mycelium"
- The hyphae have cross walls, but are perforated allowing free passage of nuclei and cytoplasm
- There are three main types of fungi; Mold, Mushrooms and Yeast
Fungal Infections
Fungi can act as pathogens, causing a number of diseases in plants and animals. Because mushrooms are more genetically similar to animals than other organisms they are often very difficult to treat.
Mycotic (fungal) infections pose an increasing threat to public health for several reasons. The scientific and medical staff of the Mycotic Diseases Branch is involved with prevention and control among three broad categories of fungal infections:
- Opportunistic Infections such as cyrptoococcosis and aspergillosis are increasingly problematic due to the rise in number of people with weakened immune systems
- Hospital associated infections such as candidemia are leading cause of bloodstream infections in the US. Changes in healthcare practices can provide opportunities for new and drug-resistant fungi to emerge in hospital settings
- Community-aquired infections such as Valley fever, blastomycosis, and histoplasmosis are caused by fungi that are abundant in the environment. Climate change may effect their growth
Protozoa
Protozoa are single-celled eukaryotes that ingest food (algae and bacteria) by phagocytosis and generally move via pseudopods (flowing extensions of the plasma membrane) or a whip-like flagella. Most are too small to be seen with the naked eye. They reproduce by fission.
- Phagocytosis is the process of by which a single cell engulfs and ingests particles or other cells to form a phagosome or food vacuole, which is a membrane-bound spericale vacuole that forms by pinching off from the cell membrane. The phagosome can fuse with a lysosome, which is another membrane-bound vacuole that contains digestive enzymes, to form a phagolysosome, which digests the engulfed material. The product can be used for energy or synthesis of other compounds and unused debris can be ejected via exocytosis.
- Binary Fission is a form of asexual reproduction and cell division used by all prokaryotes and some organelles within eukaryotes.
Animal-Like Protista
There are a number of protozoa that inhabit the gastrointestinal tract of humans. Most are harmless or cause only mild problems, but others cause serious disease. Many protozoa infections are transmitted via the fecal-oral route, while others are transmitted via insect vectors (e.g. malaria) or STD. Some have fairly complex lifecycle that may include a cyst stage to remain dormant in the environment for a period of time until a new host is acquired.
Malaria Life Cycle
Malaria is caused by infection with one of several species of protozoa called Plasmodium. The lifecycle is complex but note there is no animal reservoir. It is transmitted from human to human by mosquitoes, so it may be possible to eradicate.
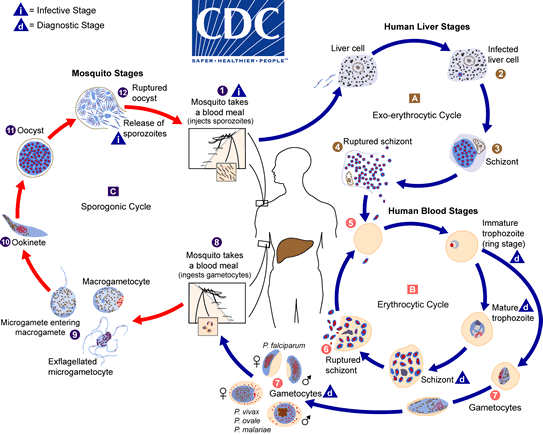
Plant-Like Protozoa
Ex. Karenia vrevis algae blooms are red algae formed as a result of nutrient pollution.
Animal-Related Infections
Helminths are large multicellular organisms that are generally visible to the naked eye in their adult stages. Like protozoa they can be either free-living or parasitic in nature. Ex. tapeworks, hookworms. Most of these infections occur in warm cllimates and effect poor communities, with more than 1.5 billion infections a year (1 in 4 people). These spread through the soil and can be carried through feces.
Anthropods are blood sucking parasites that refer to organisms that attach or burrow into the skin for relatively long periods of time (ticks, fleas, mites, etc). Antropods are important in causing diseases in their own right but are even more important as vectors or transmitters.
Non-Living Infectious Agents
Scientists generally agree that there are 5 requisite characteristics of living organisms:
- Have one or more cells with DNA
- Are capable of reproducing, growing and developing
- They are capable of capturing & using energy & raw materials
- They are able to sense & respond to the environment
- They are capable of evolving over generations
There are two agents of disease which do not fit into these categories: Viruses and Prions.
Viruses
Viruses are assembles of organic molecules that consist of some short strands of RNA or DNA encapsulated within a protein shell. In a sense, they represent a primitive assembly of organix molecules that resemble living cells yet do not meet the characteristics and complexity needed to be truly living organisms. All viruses are parasitic because they need a living host cell in order to replicate.
Once a virus binds to a living cell they can use a host's cellular energy and machinery (ribsomomes) to replicate its genetic material and its proteins to self-assemble new virus particles. These can lie dormant or can cause the host cell to rupture and release particles to infect other host cells.
Viruses can infect all kinds of living cells, including bacteria, and almost all viruses are pathogenic. When a virus infects a host cell they can cause disease through several mechanisms:
- Weakening a cell's membrane or lysosomal membranes leading to lysis of cell
- Triggering the body's immune system to attack and destroy virus-infected cells
- Provoking such a strong response from the immune system that the response itself damages or kills the host
- Weakening immune function (e.g. HIV)
- Synthesizing viral proteins that interfere with host cell function (e.g. HPV)
DNA Viruses
Viruses that contain short strands of DNA (herpes, varicella, human papilloma virus) attach to specific human cells via proteins on their surface. The cell membrane then engulfs the virus giving it access to the cell's interior where it uses the host cell enzymes to replicate its DNA, transcribe the DNA to make messenger RNA, and then translate the messenger RNA into viral proteins. The replicated DNA and viral proteins are then assembled into complete viral particles and the new viruses are released from the host cell. In some cases, virus-derived enzymes destroy the host cell membranes, killing the cell and releasing new virus particles. Other times, the new virus particles exit the cell by a budding process, weakening but not destroying the cell.
RNA Viruses
Some viruses contain RNA in their core, such as influenza infection. The protein on the exterior of the shell binds to a protein on the host cell, triggering the host cell to internalize the virus. The virus then sheds its protein coat and releases RNA into the cell. The viral RNA is used a messenger RNA to produce viral proteins. In this process, the host cell's ribosomes, amino acids, and ATP are used to create new viral proteins. Once there is a critical mass of new viral proteins and RNA, they self-assemnble to form new viral particles that are released from the host cell by budding off or rupturing. and infect additional cells.
Other RNA viruses called retroviruses use an enzyme called reverse transcriptase to copy the RNA genome into DNA. The DNA then integrates itself into the host cell genome. These viruses frequently exhibit long latent periods in which their genomes are faithfully copied and distributed to progeny cells each time the cell divides. The HIV virus is a familiar example or retrovirus.
Patterns of Viral Infection
Prions
"Protein Infection Particle" or Prion diseases have been with us for some time but only came to attention of the general public during the 1970's. Prion proteins are normally found in all mammalian brains but it is believed that altered forms of these proteins fold abnormally as a result of mutations that cause the proteins to fold into abnormal shapes that prevent them from being broken down by normal remodeling processes.
In 1997 Stanley Prusiner was awarded a Nobel Prize for his hypothesis that a mutant prion is an abnormally folded prion protein (PrPSc) that is resistant to heat & sterilization and does not evoke an immune system response. The protein is chemically the same but folds differently. The abnormal protein contacts normal proteins in neural tissue and induces them to refold into an abnormal confirmation as well. refolded molecules induce the same change in still more proteins. The abnormal proteins resist degradation and accumulate in neural tissue causing damage.
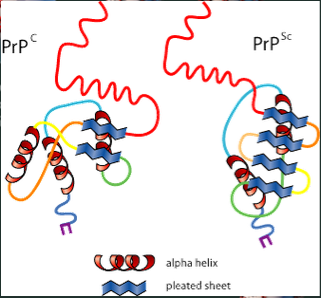
The above illustration represent a normal protein on the left (PrPc) and an abnormal on the right (PrPSc). The abnormally folded protein has segments folded into "beta sheets" (the segments with green arrows). These segments tend to stick together causing clumps of proteins that resist breakdown. Over time the clumps grow larger and destroy nerve cells in areas of accumulation leading to progressive neurological symptoms.
The Biology of a Pandemic
The COVID-19 pandemic which began in late 2019 has been truly devastating event that has caused not only widespread illness and death, but disruptions in virtually all human activities.
COVID-19 is the disease caused by the coronavirus SARS-CoV-2. The Coronaviruses are a large family of viruses that can infect mammals and birds causing diseases that range from mild colds to acute respiratory syndromes (hence SARS) and death. The term "coronavirus" comes from the spike proteins that radiate from the external envelop (corona=crown).
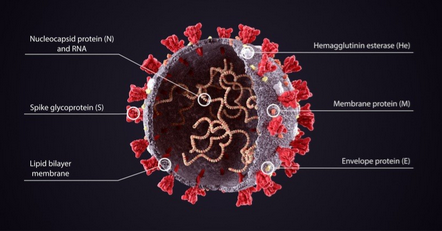
The envelope consists of spike proteins sticking out of a lipid shell that encloses the single RNA genome and some proteins.
The virus enters the body through the mouth or nose, and fuse with a specific proteins on the surface of a cell and inject their RNA genome into the cell. The cell's ribosomes translate the virus's RNA into proteins including RNA polumerase which transcribe the virus's RNA, making more RNA copies that are translated into proteins and more copies of the genome. Then the genome and proteins combine to make a new virus packaged into an envelope formed from the cells membranes. Newly formed cells travel to the cells surface and are released outside the cell, where they can infect other cells or leave the body in mucus and saliva droplets.
By the Numbers
Death Rate
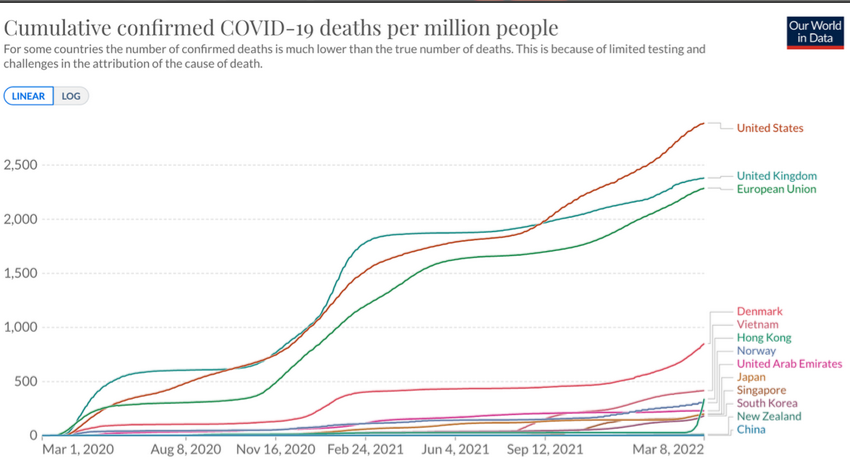
The COVID-19 pandemic emerged in 2019 and as of April 2022 is estimated to have caused illness in 500 million people globally and killed more than 6 million. Note how widely the death rate varied from country to country and how the rate declines and surges due to mutations of the viral genome. The factors responsible for these variations are not completely understood, but several major factors have been identified.
Basic Reproductive Number (R0)
Viruses differ in their inherent contagiousness and and in the absence of any preventive measures the contagiousness of a virus or bacterium is estimated as a quantity called R0 ("R naught").
R0 is a measure of the average number of new cases caused by an infected person in a population with no immunity.
Ex. If R0=3 one infected person would infect 3 more people to become infected on average. Each of those 3 infect 3 more and etc, resulting in an exponential increase.
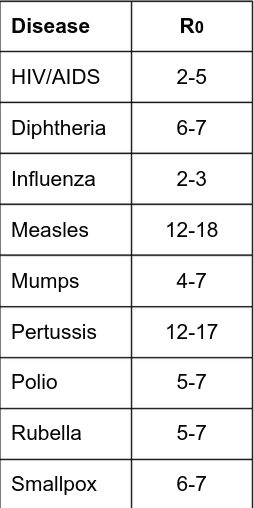
At the beginning of the pandemic everyone was susceptible and early estimates of R0 were around 2.2-2.7; causing a rapid increase in cases.
The Effective Reproductive Number
The basic reproductive number was relevant at the beginning of the pandemic because no one was immune and no control measures had been instituted. However the reproductive number has changed over time, partly because people who were infected and have immunity for a while. In addition, the probability of transmission of a respiratory virus or bacterium may be influenced by other factors such as:
- Immune Status
- Frequency of contact with others
- Duration of contact
- Proximity of contact
- Ventilation
- Wearing an effective mask
- Hand Washing
- Climate and seasonal variation
- The duration of disease in infected persons
- COVID testing and contact tracing
- Isolation and Quarantine
- Availability and utilization of effective vaccine
Seasonal variation is beyond our control, but the other known factors provide opportunities for interventions that can reduce the effective reproductive number.
If the effective reproductive number remains greater than 1 an epidemic or pandemic will continue. If interventions reduce the effective reproductive number below 1 and keep it there it will eventually disappear.
In absence of any intervention, diseases like COVID-19 can spread rapidly in a susceptible population.
The US and most of Europe experienced much higher morbidity and mortality rates compared to countries such as China, Japan, South Korea, and New Zealand which adopted rigorous social distancing measures. These measures prevented the early exposure surge and when relaxed the rates of infection rebounded.
Vaccines and Heard Immunity
If this can be achieved, the opportunities for transmission to susceptible people become diminished to the point that propagation of the virus cannot be sustained. When this is achieved, even susceptible persons enjoy a significant degree of protection.
The fraction of a population that must be immune (by being vaccinated or by recovering from infection) to achieve heard immunity can be estimated by [1 - (1/R0)]
Ex. For a typical strain of influenza A with R0 = 2.5, it would be desirable to vaccinate at least 1 - 1/2.5 = .6 or 60% of the population. Since R0 for COVID was in this range early in the pandemic, this was the goal that many articulated when vaccines began development.
Highly effective vaccines against COVID-19 became available in Dec 2020. Many people were eager to get it at first, but after a while vaccinations slowed due to vaccine hesitancy. As of April 2022, only ~66% of the US was fully vaccinated. This would have been sufficient if the R0 was still 2.4 but unfortunately mutations produced more transmissible strains such as the Delta strain with R0=5.08, and Omicron with 8.2. Achieving herd immunity against Omicron would theoretically require a vaccination rate of 88%.
Testing, Case Investigation and Contact Tracing
Many people infected with SARS-CoV-2 have minimal or no symptoms but can still transmit the disease to others.
In addition to promoting vaccination, another important strategy is abundant testing to identify symptomatic and asymptomatic cases in order to isolate them until they are no longer effective. Also, contacts of infected people should be traced and counseled regarding quarantine and what steps to take if symptoms develop.
Viral Mutations
When viruses replicate, random mutations occur occasionally. These may increase or decrease the transmissiblity or adverse effects of the virus, or have no effect. The more a virus replicates, the more likely that strains with altered properties occur. One consequence of not controlling the pandemic quickly is that viral replication continued at a staggering rate that is increased the probability of generating more transmissible strains.
COVID-19 Accentuates Inequities
Health equity means equal distribution and access to health resources for all people. It is strongly influenced by social determinants of health such as neighborhood, health care, work conditions, income, wealth, and education.
The CDC notes some racial and ethnic groups have been disproportionately effected by COVID-19 due to longstanding disparities in these determinants. Many politicians are noting that black people have more underlying medical conditions but they're not explaining why. They blame the choices made by black people or poverty or obesity - but never racism.
Communities of color are often redlined into housing with crowded neighborhoods with less access to public transportation, nutritious food and quality health care. These groups are also less likely to have health insurance and access to care. In addition, they disproportionately work in "essential" non-remote work settings such as health care, factories, food production, sales and public transportation. These workers generally also have lower incomes, less wealth, less paid sick leave, and more debt.
Medical and public health institutions have repeatedly violated the trust of communities of color through historic injustices including mistreatment and racism within public health and healthcare, leading to a well-earned skepticism of new interventions such as the COVID-19 vaccines. It was initially assumed people of color were accessing vaccines less but as of April 2022 this trend has changed, some communities of color have high vaccination rates than their white neighbors.
The life expectancy declined in all income groups during the pandemic but the poorest 20% which already had the lowest life expectancy had the greatest decrease.
Respiratory Health
All animals need oxygen to metabolize nutrients to generate cellular energy.

The above equation illustrates how nutrients (glucose) are converted to cellular energy in the form of adenosine triphosphate (ATP). Note carbon dioxide is produced as a by-product of metabolism.
The lungs are the interface between our blood stream and the external environment and the site where O2 is taken up and CO2 leaves the bloodstream to be expelled into the environment. The intimacy of this interface between our internal and external environment with the need to exchange air has a major impact on health for several reasons:
- Continual exposure of the respiratory tract to air from the environment provides an important portal for entry of viruses and bacteria that can cause infection.
- Disease processes that impede the mechanisms of ventilation (e.g. asthma and emphysema) can cause severe illness or death; these processes can also be triggered or exacerbated by substances in the air we breath.
- Air is a variable and complex mixture of many substances including particulate matter and chemicals that can have a detrimental effect on lung function; moreover many of these chemicals can be absorbed into the blood and cause a wide range of health problems.
Learning Outcomes
- Describe the function of alveoli with respect to exchange of oxygen and carbon dioxide
- Describe the role of hemoglobin in oxygen transport and the adverse effects of CO
- Explain how the occurrence and severity of chronic obstructive pulmonary disease (COPD) and asthma relates to environmental factors and be able to give examples of factors known to trigger asthma attacks
- List the six criteria air pollutants and discuss the impact of air pollution on health
- Discuss the impact of environmental tobacco smoke on health
The Respiratory Tract
Inspired air enters through the nose or mouth, passes through the pharynx (throat) and larynx (voice box) and then enters the tracheo-bronchial tree. The trachea bifurcates into the rate and main stem bronchi which branch again and again into increasingly smaller conduits called bronchioles.
Respiration continually brings air from the environment in contact with the delicate cells in our lungs to provide oxygen and to expel carbon dioxide. The air must be warmed, moistened and filtered for the lungs. When harmful contaminants are carried in the air there are several mechanisms to mitigate the effects of these contaminants.
Nasal hairs and mucus can trap dust and other particulate matter, and goblet and ciliated cells work in tandem to remove particulate matter. Goblet cells create a mucus layer on the lining of the surface that protects the cells and traps dust and other foreign material while ciliated cells have hair-like projections that move rhythmically and sweep the mucus and particulate matter upwards where it can be swallowed or expectorated.
Supplying Oxygen and Expelling CO2
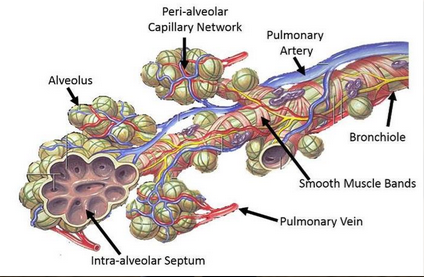
The above figure shows a bronchiole terminating in several clusters of bronchiole. The bronchiole has a vacular supply of oxygenated blood (in blue) and nervous enervation (nerves in yellow) and the bronchiole is wrapped by smooth muscle cells that can contract or relax in response to physiologic conditions.
Contraction of smooth muscle narrows the airways, and relaxation increases their diameter. Abnormally severe contraction of this smooth muscle is of central importance to asthmatic attacks.
Eventually, the terminal bronchioles open into thousands of alvelo - delicate grape-like clusters of air sacs where gas exhange occurs. There are several types of alveolar cells: type 1, type 2, and macrophages.
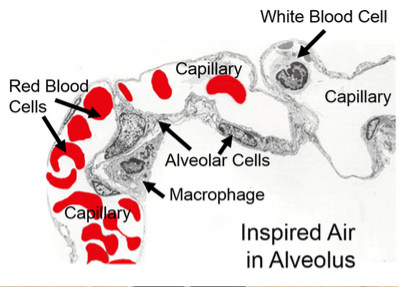
The above image focuses on the details in a single alveolus. Note the capillaries surrounding the alveolar cells are in very inimate contact, which facilitates the exchange of oxygen and carbon dioxide between the air in the alveolus and blood in the capillary.
The alveolus is lined with alveolar cells; type 1 are for exchange of O and CO2, while type 2 can divide to give rise to new type 1 cells and also synthesize and secrete a substance called surfactant which reduces surface tension in the alveolus and prevents collapse during expiration.
Within the alveolus there are also macrophages (also called "dust cells") - phagocytic cells that engulf particulate matter then migrate up the bronchioles where the ciliated cells sweep them up into the pharynx where they are swallowed or expelled.
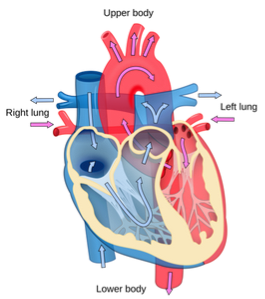
The graphic above illustrates that blood returning to the heart is de-oxygenated (in blue) and returns to the right atrium of the heart and then the right ventricle. When the heart contracts blood in the right ventricle is pumped to the lungs where it enters capillary vessels that circulate around the alveoli where gas exchange takes place. As blood circulates around the alveoli it becomes re-oxygenated and CO2 moved from the pulmonary arterial blood into the alveolus to be exhaled. Blood returning to the left atrium of the heart then to the left ventricle is fully oxygenated and when the heart contracts it is pumped into the aorta to be distributed throughout the body via the arterial system.
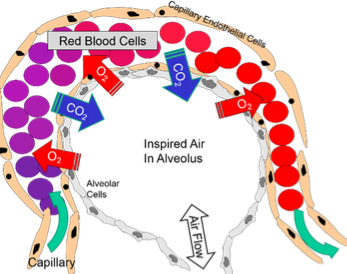
Blood returning from the peripheral tissues has a relatively low concentration of oxygen but is rich in CO2 as a result of cellular metabolism. As a result, the oxygen readily diffuses from the alveolus across the alveolar cells and into the capillary where it binds to the hemoglobin in red blood cells. Conversely, CO2 diffuses from the capillary blood into the air in the alveolus which is exhaled.
Cellular Gas Exchange
Cells use oxygen to metabolize, or create cellular energy from glucose or fatty acids. Arteries branch into arterioles which eventually branch into capillaries.
The image above shows an arteriole branching into smaller capillaries which supply nutrients and red blood cells to metabolizing cells. Capillaries are often so thin that often red blood cells can only pass one at a time.
Smoking
Tobacco smoke is a complex mix of toxic and carcinogenic chemicals and particulate matter. Emission levels of 98 components in mainstream smoke constitute a human inhalation risk with potential to contribute to many adverse effects.
Below is a list of some of the known effects:
- Cancer of the bladder, blood, cervix. colon, esophagus, kidney, larynx, liver, oropharynx , pancreas, stomach, trachea, bronchus, or lung
- Generates free radicals that damage tissue membranes
- Increases blood pressure and clotting
- Promotes atherosclerosis
- Causes 2 to 4 fold increased risk of coronary heart disease; Including stroke and peripheral vascular disease
- 12 fold increased risk of COPD
- Heavy smokers have a 20 fold risk for lung cancer
- Many maternal/fetal effects
- Nicotine and free radicals kill osteoblasts - bone-making cells
- Older people who smoke experience significant bone loss
- Smoker's bones take longer to heal and may experience more complications during healing
- Second hand smoke puts non-smokers at risk
Since carbon monoxide from smoke binds to hemoglobin in red blood cells, effecting delivery of oxygen and causing platelets to become stuck together causing blood clots, thus every organ is effected by smoking. In addition, nicotine and CO can damage the inner lining of arteries. In coronary heart disease plaques can reduce or block flow of blood to the heart, causing chest pain. In more serious cases when the heart muscle is starved of oxygen for too long an area of the heart may die, causing a heart attack.
Smoking is the leading preventable cause of death in the US. More than 480,000 deaths per year can be attributed to cigarette smoking. Smoking causes 90% of lung cancer deaths. While COPD is more common in men, more women die from COPD annually. More women die from lung cancer each year than breast cancer. About 50-80% of all deaths from COPD caused by smoking.
COPD
Chronic Obstructive Pulmonary Disease (COPD) is a global health problem that effects millions of people. COPD is one of the top 10 causes of death worldwide and the direct cost of treating it in the US alone is ~$30 Billion per year.
Symptoms
- Shortness of breath
- Wheezing
- Chest tightness
- Difficulty with routine activities
- Weight loss
- Fatigue
COPD actually represents a spectrum of disease ranging from destruction of the alveoli and thickening of the terminal airways and impaired airflow (emphysema) to the thickening of the airways with chronic inflammation and repeated bouts of infection (chronic bronchitis). The hallmark of COPD is reduced airflow, which occurs as a result of one or more of the following:
- Loss of elastic recoil in the alveoli due to excessive breakdown of the protein elastin
- Destruction of the walls between the alveoli as a result of excessive action of enzymes called "proteases"
- Thickening of the walls of the airways due to inflammation
- Excessive secretion of mucus, which can clog airways.
While smoking is the leading cause of COPD, it can also be caused by genetic or environmental factors. Respiratory infections such as influenza do not cause COPD, but can make it much worse.
Asthma
Asthma is a common, chronic syndrome characterized by intermittent episodes of symptoms which can be severe and life-threatening. The clinical episodes are triggered by antigens, viruses, exercise, or inhalation or irritating substances. Any of these stimuli can trigger a hyperactive allergic response which produces:
- Inflammation of the respiratory tract
- Bronchoconstriction
- Hypersecretion of mucus
These can cause varying degrees of airflow obstruction causing shortness of breath, wheezing, coughing, tightness in chest, and some times sever "air hunger" panic. Some episodes resolve spontaneously, while others require medical treatment.
The CDC estimates nearly 20 million Americans have asthma, and it is more common in children than adults, more common in women than men, and more common in black people than white people. The mortality from asthma rose in the 1980's, but then plateaued and declined since 1999 due to improved treatment.
Why do some people have seasonal allergies?
Seasonal allergies are a hyper-sensitive immune response to something that's not actually harmful. Pollen or some allergen finds it's way into the mucus membrane and the immune system attacks it. When the white blood cell attaches to the allergen it releases a chemical which simulates nerve cells and cause blood vessels and the mucus membrane to swell and leak fluid; itchiness, sneezing, congestion, etc. An allergy can even bring on full anaphylaxis.
Asthma Triggers
- Allergens (pollen, dust, molds, animal dander, bugs, etc)
- Tobacco smoke
- Exercise/activity (especially in cold air), as well as laughing, crying, or hyperventilating
- Cold air, wind, rain, and sudden changes
- Medications
- Air pollutants and irritants
- Sinusitis - respiratory tract infections including the flu and common cold
- Sulfities (preservatives added to some perishable foods)
- Emotional Stress
Environmental Remediation for Asthma
The medical management of asthma and treatment of acute attacks has improved substantially, but the prevalence of asthma continues to rise in urban settings in industrialized countries. There is some evidence that interventions to reduce trigger exposures are effective, but the literature indicates that allergen reduction is difficult to achieve and the effectiveness is not as great as expected.
Air Pollution
Air pollutants are the particles, vapors, and contaminants not found in pure air. These primarily come as a result of burning hydrocarbon fuels and releasing by-products into the atmosphere. Pollutants can be naturally occurring or the result of human activity (anthropgenic).
The energy humans require for energy is mostly derived by combustion. Combustion involves oxygen combining with hydrocarbons (gas, oil, propane, natural gas, wood, etc) to produce energy. The by-products are CO2 and CO, water vapor, smoke, and ash. CO tends to be formed when there is insufficient oxtgen for the hydrocarbon to burn completely.
Combustion of hydrocarbon fuels also produces "particulates" some of which are visible as smoke. These can pose treats to health and the environment. Nitrogen is the most abundant gas in the air we breathe, and it to combines with oxygen during combustion to form a series of compounds called nitrogen oxides, sometimes referred to as NOx. Sulfur dioxide SO2 is also formed at combustion of surfer-containing fuels such as coal. Other pollutants can also be released by combustion, coal also contain concentrations of mercury which gets turned into vapor and returns to our waterways driving concern about mercury in the ocean. Polycylic aromatic hydrocarbons (PAH) represents a large family of molecules can also be produced when dirty fuel is burned, which cause tumors and birth defects.
DNA, Heredity and Drug Resistance
Chromosomes are molecules of DNA that provide the essential genetic code for all living organisms, and it is the code that directs the synthesis of proteins that define each organism's structure and function. Genetic factors contribute to causation of many diseases, such as breast cancer and heart disease. Understanding genetics also enables one to understand the major threats to health as a result of the development of drug resistance.
Learning Outcomes
- Explain how DNA encodes genetic information and the role of messenger RNA and transfer RNA
- Explain how DNA directs protein synthesis and roles of DNA and proteins in regulating cell function
- Demonstrate how to predict the possible genotypes that could occur in an offspring provided one knows the genotype of both parents
- Explain what a mutation is and give examples of how it might occur
DNA
Deoxyribonucleic acid (DNA) is an extremely long polymer made from units called nucleotides.
The backbone of each molecule is composed of alternating sugars (the pentagon with "S") and each sugar is also covalently bonded with one of the following nucleotide bases:
- Adenine (A)
- Thymine (T)
- Cystosine (C)
- Guanine (G)
- Uracil (U)
DNA and RNA differ in several ways:
- DNA is double stranded, while RNA is single stranded (though RNA forms loops by hydrogen-bonding to itself)
- DNA contains the sugar deoxyribose while RNA has the sugar ribose
- RNA contains the base uracil in place of thymine
The illustration above shows the 46 chromosomes that contain the human genome. There are 22 homologous pairs and 2 sex chromosomes in humans. Sex chromosomes are XX in females and XY in males. The XY chromosomes are physically different from one another in that the Y chromosome is much shorter, only containing about 9 gene loci that match those on the X chromosome. This means that, except for the sex chromosome, each gene has one chromosome is inherited from one's mother and one from the father. Each chromosome is a single molecule of DNA.
Since Y chromosomes are much shorter than those on the X chromosome, almost all of the alleles on a male's single X chromosome are expressed since there is no alternative dominant allele to mask them. This results in a distinct inheritance patter for traits that are encoded on the X chromosome. For example, color-blindness is a defective allele always carried on the X chromosome.
With the exception of red blood cells (which lost their nucleus) each cell in the human body has all 46 chromosomes, so there are about 3 billion base pairs. The single chromosome of a bacterium is located diffusely in the cytoplasm, but chromosomes of higher species are contained with a membrane-bound nucleus. If we were to take the physical human chromosome and stretch it out, it would be about 5 centimeters, or all 46 would be about 2 meters laid end to end.
One of the helical strands of DNA is the coding strand. The coding strand of a chromosome has thousands of genes along its length (segments which contain genetic code for specific cellular proteins).
Genes and Inheritance
Each chromosome contains thousands of genes. This takes up up only 3-5% of our DNA, while the rest of DNA is considered "non-coding areas." Altogether 23 pairs of chromosomes carry the code for 20k-25k genes. Most genes are transcribed into "messenger RNAs" (mRNA) that provide a template that is used to translate the code into specific proteins. About 100 genes are transcribed into "ribosomal RNAs" and "transfer RNAs" that also play a vital role in the synthesis of proteins.
The sequence of bases in DNA can be though of as "letters" that provide the basis for all genetic code for proteins synthesized by our bodies, which provide the basis of structure of all our cells, enzymes and our traits and characteristics. The production of cellular proteins requires two major processes: transcription followed by translation.
Transcription and Translation
Transcription occurs in eukaryotic cells within the nucleus where DNA is used as a template to create mRNA with the help of RNA Polymerase. The initial transcript has coding segments (exons) and alternating non-coding segments (introns).
Splicing happens in 3 stages: Initiation, elongation, and termination. During initiation the polymerase binds to the promoter region of the template, the DNA "unwinds" and opens. During elongation the polymerase links complimentary bases to the new RNA molecule until it reaches the termination part of the gene and the polymerase and mRNA strand dissociate from DNA.
Before the mRNA leaves the nucleus the inrons are removed from the transcript by a process called RNA splicing. Extra nucleotides are then added to the ends of the transcript; these non-coding "caps" and "tails" protect the mRNA from attack by cellular enzymes and aid in recognition by ribosomes. Helper proteins assemble at these caps and form a splicing machine, or splicisome. It brings exons close together and cuts the intron loop off before disassembling. Then in translation, which occurs in the cytoplasm of the cell at the ribosomes, the information in mRNA is used to create a polypeptide.
Alleles
The sequence of bases in the human genome is remarkably similar from person to person, but over hundreds of years of evolution mutations have been introduced to the human gene pool. Some are fatal, while others are passed down between generations, and they provide the basis for many variations in phenotype that make us all special. Over time, mutations have created variants of genes that are responsible for differences in the color of our hair, eyes, skin, how fast we can run, height, etc. Mutations introduce gene variants that encode for slightly different proteins, which in turn influence all aspects of our phenotype. Note though, that an individual's phenotype is not solely the result of their genome, and could be a result of interaction with their environment.
Mutations have introduced gene variants that encode for slightly different proteins, influencing all aspects of our physical characteristics (phenotype). When mutations create variants of a particular gene the alternative gene forms are referred to as alleles. Some genes have a few alleles, while others have many.
Recall also that chromosomes come in pairs with the same gene in both members of a given pair. The two genes together can be referred to as the genotype. Genes are either dominant or recessive, and dominant genes are chosen. Also, different genotypes can create the same phenotype and blending a phenotype can occur with 2 dominant traits. Punnett squares are used to determine gene dominance.
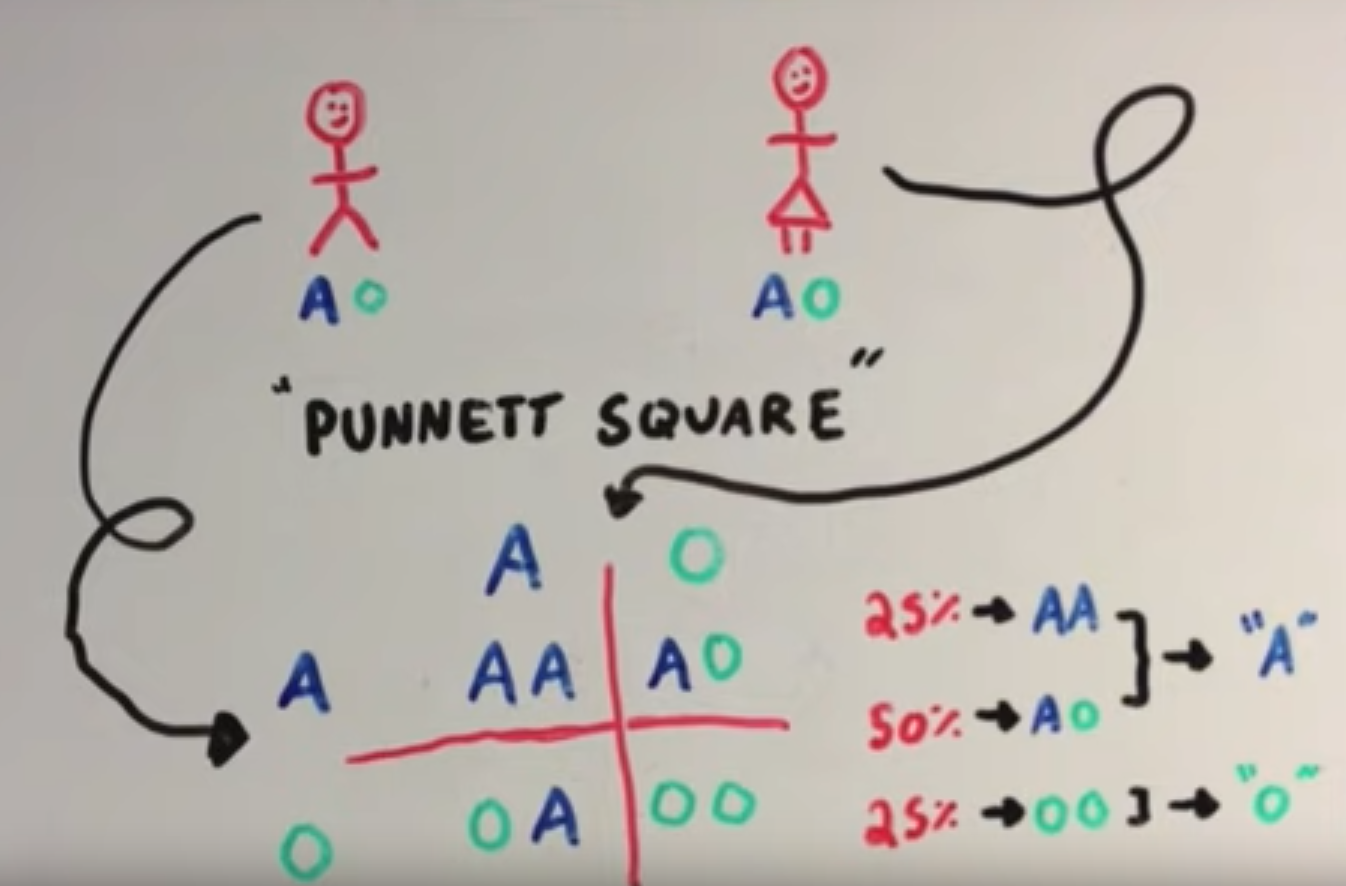
There is an allele that contains genetic code for blood type. In the above A is the dominant trait and O is a regressive trait. A person can have 2 alleles for the same blood type, which is called homozygous, and they would have that blood type. Alternatively, a person could have an A and an O blood type allele, called heterozygous, and the dominant allele would win.
Dominant vs Recessive Inheritance Patterns
Some diseases are inherited, and the pattern of appearance within a family tree will depend on whether the faulty allele is dominant or recessive compared to the normal allele.
For example, the allele for Huntington's disease is dominant. If a man with a heterozygous Huntington's disease gene (Hh) has children with a woman with no Huntington's Disease gene (hh). Their children will have a 50% chance of having the disease. When diseases have dominant alleles it will occur quite frequently in the family tree.
In comparison, cystic fibrosis is caused by a recessive allele, meaning that individuals who are heterozygous for the gene (Cc) will not manifest signs or symptoms. As a result the cystic fibrosis allele can be passed along a family tree with only sporadic appearance of the disease.
Binary Fission
Prokaryotes reproduce by the relatively simple process of binary fission. The single chromosome replicates and each copy attaches to a different location on the cell membrane. The cell membrane then begins to invigilate and eventually separates into two genetically identical bacteria. A similar process is used to replicate mitochondria within eukaryotic cells, but the overall process is more complicated in eukaryotes.
Mitosis
Mitosis is the process by which eukaryotic cells replicate by dividing into two genetically identical cells. It is the process by which new cells are formed in the embryo and after birth, and mitosis also replaces cells that have died or shed. In humans some cells retain the capacity to divide throughout life. Benign and malignant tumors also grow through mitosis.
Meiosis
Meiosis is the specialized process by which gametes (sperm and eggs) are produced for sexual reproduction in the ovaries and testes. Each gamete has 23 chromosomes and joins with the other gamete to create a mixture of genetic information from both parents.
Meiosis produces sperm and eggs with novel mixtures of the original parental chromosomes due to:
Random Assortment - Separation of homologous pairs of maternal and paternal chromosomes results in each gamete randomly getting some maternal chromosomes and some paternal. Random assortment of 23 pairs of chromosomes can produce > 8 million possible combinations.
Crossing Over - After maternal and paternal chromosomes match up as homologous pairs they exchange sections of DNA, this further shuffles the genetic deck.
Epigenetics
Our genome is established when fertilization takes place, and the code remains unchanged throughout our life except for certain mutations that may occur in individual cells.
We now know that many external factors (epigenetics) can affect the timing of the gene expression, the degree expression, and the eventual phenotype that is expressed. These external factors can produce small modifications to DNA, such as addition or removal acetyl or methyl groups to DNA, or to the histones that control the wrapping and packing of DNA. Attachment of methyl groups appears to reduce transcription or even shut it off. attachment of acetyl groups to histones turns genes on or off.
These biological changes to the genome is known as 'epigenetic factors', changes above the level of the genome. In essence, the DNA in our cells provide the code for making functional proteins, and the epigenetic factors act as switches to turn genes on and off.
Certain genes that predispose an individual to being lean, however the individual might still become fat due to overeating.
Mutations and Drug Resistance
All humans have the same set of genes and the sequence of our base pairs in remarkably similar. However this doesn't mean we have all the same nucleotide sequence in our genome. If this were the case, then all humans would be clones having exactly the same genetic code. While DNA replication is remarkably precise, errors occasionally occur and produce changes in the base sequence.
Mutations are random changes in the sequence of base pairs in DNA and metagens are factors that cause mutations (chemicals or radiation). Mutagens result four patterns of alteration in the base sequence:
- Replacement (substitution) of a single base pair
- Addition of one or more base pairs
- Deletion of one or more base pairs
- Relocation of a segment of base pairs
Addition or deletion of pairs can be substantially disruptive, since mRNA transcript is read in 3 letter codons a shift could throw off the entire sequence.
Mutations can result in:
- Inconsequential changes which do not alter protein product
- Small changes that alter the protein product to some degree
- Small changes that alter phenotype markedly
- Very large changes in base sequence that arise from insertion or deletion of a base pair, or relocation of a segment of nucleotides.
The term ""anti-microbial" is a generall term that encompasses drugs, chemicals, or other substances that kill or slow the growth of microbes. These include:
- Anti-bacterials (antibiotics)
- Anti-virals
- Anti-fungals
- Anti parasitics
Alexander Fleming is widely credited with the discovery of penicillin in 1928, though there are earlier reports of mold killing bacteria. Penicillin became widely used, and with it resistant strains of bacteria emerged. At first these problems were dismissed but by the 1980s it had become a clear problem. Exposure to antibiotics kill susceptible bacteria, but the resistant strains spread their genes. Bacteria can also spread the strand of DNA which contains antibiotic resistance to other bacteria.
To avoid antibiotic resistant bacteria we can focus preventing infection, and appropriate use of antibiotics.
Cancer
The oldest description of cancer were written in Egypt as early as 3000 BC as part of an ancient Egyptian textbook on surgery.
The word "cancer" comes from the Greek work carcinos, which means crab. Hippocrates used this term to describe the disease because the projections of a cancer invading nearby tissues. During the 16th century, when the theory of bodily humors prevailed, it was believed cancer was caused by excess black bile buildup; But this was discarded early when no black bile was found. After invention of the microscope, evidence accumulated that cancer was the result of uncontrolled cell division but the cause was still unknown.
Learning Objectives
- Describe the distinguishing features of a cancer
- Discuss the mechanism by which cancers evolve
- Explain what is meant by "metastasis" and the mechanisms by which it occurs
- Explain the difference between the "grade" and the "stage" of a cancer
- Discuss risk factors for cancer and strategies for prevention
- Define the following terms:
- Cell differentiation
- Benign tumor
- Malignant tumor
- Dysplasia
- Carcinogen
- Proto-oncogene and onogene
- Tumor-suppessor gene (anti-oncogene)
- Apoptosis
Cancer Biology
Cancer is the result of a long process that begins when one of the cells in organs or tissue becomes damaged or altered in a way that causes it to break free from normal controls that allow cells to work in harmony. Cancer cells with divide via mitosis even if they do not receive the appropriate signals. This can lead to a mass of cells, or a tumor.
The nucleus of a cell contains the genetic information, within the chromosomes. Certain genes make products that lead cells to reproduce. The genes responsible for making cells divide are called proto-oncogenes. Changes in normal genes lead to the production of proto-oncogenes, making cells divide faster. There are also genes that stop the division of cells, known as tumor-suppressor genes (AKA anti-oncogenes). We have two of these genes (one from each parent), so if one tumor-suppressor gene is damaged, usually the other is able to stop the cell from behaving abnormally.
The process by which tumors cause the body to provide the cell with nutrients is call angiogenesis. The tumor sends out messages that say "feed me" and the nearby blood vessels send over new extensions that deliver food and oxygen. The blood vessels also act as a passageway for movement of tumor cells. The movement of tumor cells to other parts of the body is called metastatis. 90% of cancer deaths occur when the tumor spreads to different parts of the body.
One way the development of cancer is prevented is the death of defective cells. If the body is unable to replace or repair the damaged, stressed, or worn-out cells it commits cellular suicide, or apoptosis. This leads to the breakdown and death of the cell. It is estimated over 50 billion cells undergo apoptosis each day in adults, and is carefully regulated through complex mechanisms. Cancer cells lose this critical capability and lead to buildup of abnormal cells. Cancer cells can also develop resistance to drug or chemotherapy treatment in the same way bacteria might.
Cell Differentiation
A major difference between cells in a growing embryo and those in an adult is that most of an adult's are differentiated (they have become specialized in structure and function). Muscle cells are elongated and contain an abundance of contractile proteins, whereas pancreas cells are specialized for secretion of digestive enzymes.
The cells in the earliest stages of an embryo are totipotent, meaning they have the capacity to divide and give rise to any of the specialized cells in the body. In contrast, in an adult the replacement if shed or worn out cells takes place by division of somatic stem cells (also called adult stem cells), which are not fully differentiated but can give rise to only a limited array of cells.
For example, stem cells in the bone marrow (hematopoetic steam cells) and divide and give rise to progenitor cells that can differentiate into cellular elements of blood and immune system, including red blood cells, lymphocytes, platelets and more. Bone marrow stromal stem cells (mesenchymal stem cells or skelatal stem cells) can generate bone, cartilage and fat cells.
When stem cells are called upon to generate a particular type of cell, they undergo asymmetric cell division in which one of the child cells has a finite capacity for cell division and begins to differentiate and the other sibling cell remains a stem cell with unlimited proliferative ability.
New cells are born through the division of an existing cell into two through mitosis. The need for new cells continues through our entire life, but is greatest in early life. A fertilized egg divides into two cells, which splits to 4, 8, 16, 32, 64, etc... In a fully grown adult the rate of cell proliferation is much less, and under normal circumstances only takes place when signals indicate cells need to be replaced.
Cell differentiation is not completely understood, but involves the activation or inactivation of certain genes in response to the cell's interaction with neighboring cells and with its extracellular matrix (ECM). Receptors on the cell will bind to specific molecular elements in the ECM and this binding activates the intracellular signal transduction pathways that turn certain genes on or off. As a result some genes can be expressed in a given cell, and others cannot. Some cells, like sketelal and muscle cells, become terminally differentiated meaning their ability to proliferate is permanently lost, though they can continue to perform their functions.
Ex. of Normal Cell Division: The outer layer of skin (eipdermis) is about 12 cells thick. Cells in its lowermost basal layer divide just fast enough to replinish shed cells. Division of a basal cell produces one cell that remains in the basal layer and retains the capacity to divide. The other migrates out of the basal layer and loses the capacity to divide, thus the number of dividing cells in the basal layer stays roughly the same.
Ex. of Abnormal Cell Division: The transition to skin cancer begins when the normal balance between cell division and cell loss is disrupted. Basal cells divide faster than needed leading to an increasing number of dividing cells. This creates a growing mass of a tissue called a "tumor" or "neoplasm". The organization of the tissue gradually becomes more disrupted.
Benign Tumors (skin moles, lipomas) are abnormal growths that are no longer under normal regulation, but grow slowly, resemble normal cells,and still have surface recognition proteins that bind them together and keep them from invading or metastasizing.
Evolution of a Cancer
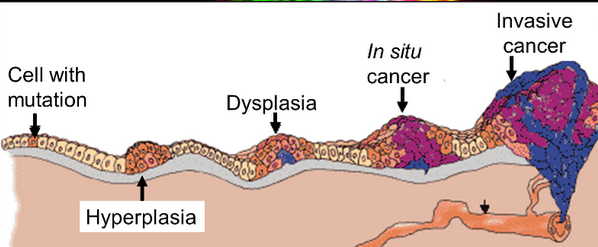
Atrophy: Reduction in cell mess
Hypertrophy: Enlargement of cell size
Hyperplasia is an increase in the number of cells in a tissue with normal cell morphology and normal cell to cell interaction
Dysplasia is a pre-cancerous state characterized by increased cell proliferation with high abnormal and variable appearance to the cells. Cell to cell interactions are diminished, and the architecture of the tissue is less organized. Dysplasia is potentially reversible and doesn't always progress to cancer, but indicates a pre-cancerous state with high probability of evolving to cancer and considered "per-malignant".
Carcinoma "in situ" literally means cancer in place. These cells have transitioned to being cancerous. In situ cancer may remain contained indefinitely, but additional mutations may occur that enable it to invade neighboring tissue and shed cells into the blood or lymph.
Metastatis is the movement or spreading of cancer cells from one tissue to another and their prolideraation at the new site. Cancer cells usually spread through the bloodstream or lymphatic system. The tumor mass can also spread locally, compress other structures and damage surrounding tissues.
Characteristics of Cancer Cells:
- Self-sufficiency in growth signals; an autonomous drive to proliferate - pathological mitosis - by virtue of the activation of oncogenes such as ras or myc.
- Insensitivity to growth-inhibitory signals; they inactivate tumor suppressors.
- Evasion of programmed cell death (apoptosis); suppression and inactivation of genes and pathways that normally enable cells to die.
Cancer Risk Factors
Radiation
Non-ionizing - low frequency, long wavelength energy which is not energetic enough too penetrate deeply or create free radicals.It only penetrates single-celled organisms and the superfical cell layers of multicellular organisms. However, it can damage DNA in superfical cells and cause mutations. UV rays from the sun and tanning salons accounts for 50-90% of all skin cancers. Ex. radio signals, microwaves, power lines, heat lamps, etc.
Ionizing - Proton, neutrons, x-rays, and gamma rays have highly energetic wavelengths enabling them to deeply penetrate tissues. Lead shields block this form of radiation. DNA can be damaged by a direct hit, but it more often indirectly damages DNA by stripping away electrons when they strike a molecule, thereby creating a highly reactive free radical. The resulting free radical can damage other molecules by stealing electrons or breaking phosphate bonds in DNA, thus giving it a cumulative mutagenic effect. Ex. Nuclear fallout, radioactive chemicals, Radon, etc.
Chemicals
A chemical carcinogen is any discrete chemical compound which has been shown to cause cancer. These can enter the body through absorption, ingestion, or inhalation. Some of these include formaldehyde, chloroform, asbestos, and arsenic. Tabaco smoke contains over 60 carcinogens.
Heterocyclic amines (HCAs) & Polycyclic Armoatic Hydrocarbons (PAHs) are a family of carcinogenic chemicals formed in cooking muscles meats (beef, pork, fowl and fish). Eggs and tofu are not associated. HCAs form when amino acids and creatine (a chemical found in muscles) react at high cooking temperatures.
Viruses
Viruses are estimated to cause 15-20% of all cancers. The host's genetic susceptibility, mutations, exposure and immune system deficiencies are also factors. Oncoviruses (cancer-causing viruses) include Epstein-Barr virus, hep B and C, HPV, and herpes. AIDs also indirectly increases risk of cancer due to impared immune function.
Consumption and Heredity
High BMI is associated with increased risk of colon, breast, kidney, esophagus, stomach, pancreas, gallbladder and liver cancer. Fat tissues produce excess amounts of estrogen, high levels are associated with some cancers. Obese people often have increased levels of insulin in their blood, which may promote the development of certain tumors. Fat cells may have a direct or indirect effect on tumor growth regulators.
Alcohol intake is associated with an increased risk of cancer of the mouth esophagus, pharynx, colon, and liver.
Most cancers are sporatic, and have to hereditary predisposition. However, there are some which can be hereditary such as Retinoblastoma, breast cancer, and colon cancer.
Heart Health
Atherosclerotic disease is a global health problem. Cardiovascular disease is the number 1 cause of death worldwide, claiming 12 billion lives annually in developing countries. In the US heart disease claims about 800,000 deaths per year. It is estimated 80% of deaths from cardiovascular disease worldwide occur in low-income and middle income countries. The high mortality is partly due to lack of access to care in many areas, but the problem will not be solved by better medical care.
Atherosclerotic is a complex process by which arteries become progressively narrowed, impairing the supply of oxygen. Impaired blood flow can result in ischemia and cause angina or intermittent claudication. Plaques can also rupture, triggering acute formation of a clot and abrupt loss of blood supply to tissues, resulting in an infarction.
Eventually, progression of atherosclerosis generally can manifest itself in three ways:
- Coronary artery disease
- Cerebrovascular disease
- Peripheral artery disease
Learning Outcomes
- Define atherosclerosis and describe the basic mechanism by which it develops, including response to injury theory
- Compare and contrast the terms ischemia and infarction
- Explain the mechanisms by which poorly controlled diabetes and hypertension contribute to heart disease
- Discuss the risk factors for atherosclerotic cardiovascular disease
The Cardiovascular System
The primary function of the heart and blood vessels is to transport oxygen, nutrients, and byproducts of metabolism. Oxygen and nutrient-rich blood is delivered to tissues via the arterial system which branches into smaller and smaller blood vessels; from arteries to arterioles to capillaries (where most exchange occurs).
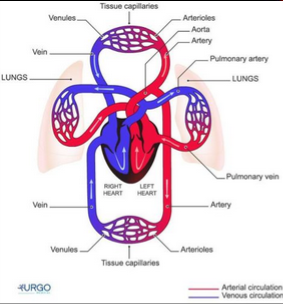
The heart is a discrete organ which has 4 chambers (in humans). Two chambers on the right side (right atrium and right ventricle) receive blood returning from the periphery and send it too the lungs for re-oxygenation. Blood then returns on the left side via pulmonary veins. After entering the left atrium blood enters the left ventricle and is pumped back into the aortic arch for distribution to the body.
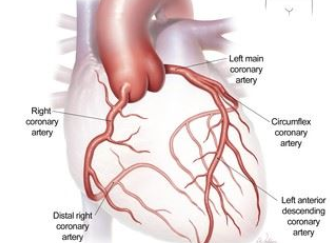
Note also that the heart requires a continuous supply of oxygen an nutrients, just like any other tissue. The heart receives its blood supply from coronary arteries which arise from the root of the aorta.
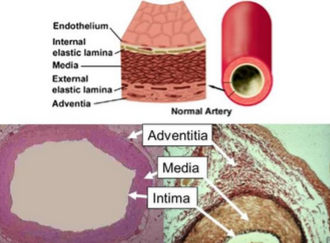
All blood vessels (arteries and veins) have 3 primary layers: Intima, media, and adventitia. Normally, the walls of an artery are smooth to allow unobstructed blood flow. The innermost layer. intima, is lined with indothelial cells which are in direct contact with blood.
Atherosclerosis
The endothelial cells that line blood vessels provide a semi-permeable barrier that regulates exchange between blood and tissues. Endothelial cells also regulate a number of less obvious processes. They provide a unique surface that generally allows the cellular elements of blood to flow without adhering too the vessel lining unless something has perturbed the cells. When perturbation occurs, these cells secrete cytokines that trigger and maintain an inflammatory response. Endothelial cells also regulate constriction and relaxation of vessels by releasing vasodilatory molecules and vasoconstrictive molecules.
Atherosclerosis occurs when plaque builds up in the arteries. Enough can eventually lead to a heart attack or stroke. Atherosclerosis can be asymptomatic in its early stages but become serious as blood supply becomes compromised. It starts with damage to the artery wall, then calcium and blood cells begin to build on the damaged wall. Chemical reactions occur with LDL Cholesterol triggering inflammation and cells release a chemical SOS signal and white blood cells begin to eat the cholesterol, which cause the cells to turn to foam and turn to plaque.
Risk Factors
There is a direct link between risk of cardiovascular disease and concentration of cholesterol in the blood. Cholesterol is a waxy, fat-like substance that's found in all the cells in your body. Your body needs some cholesterol to make hormones, vitamin D, and substances that help you digest foods. LDL is the "bad" cholesterol that sticks to your arteries. Satins are currently the most powerful cholesterol lowering drugs, inhibiting the synthesis of cholesterol in the liver. HDL is the "good" cholesterol; Blood levels of HDL are inversely related to risk of coronary artery disease.
Obesity is associated with some cancers, Type II diabetes, hypertension, and heart disease. BMI is usually used to measure fatness, but can be inaccurate because it does not take into account muscular development or fat distribution. "Central adiposity" is fat deposition in the torso (the "apple-shaped" person) which is more indicative or cardiovascular risk.
Type 1 and 2 diabetes are risk factors for CAD. People with diabetes cannot produce insulin, which circulates in the blood and binds to insulin receptors on the muscles and fat cells triggering insertion of specialized glucose transporters to facilitate the entry of glucose from the blood to the cell.
Other factors:
- Smoking - smoking is really bad mmmkay
- Alcohol consumption - almost all studies have concluded that moderate alcohol consumption is associated with 20-40% lower incidence of CAD, compared with non-drinkers or heavy-drinkers. However, there could be an unknown confounding variable.
- Gender differences - Women tend to develop heart disease about 10 years after men
- Aspirin and Vitamins - A study in the 1900's suggested there may be a 30% risk reduction of myocardial infarction by taking aspirin.
Factors Related to Human Health
Social, Political and Economic
There is growing recognition that there are many social determinants of health. To fully understand the impact on health we must recognize a persons character and environment. The WHO categorizes these determinates as Structural and Intermediary. Structural determinants refers to socioeconomic and political context such as governance, polices and values which lead to an unequal distribution of material and monetary resources, changing their socioeconomic position. Intermediary determinants are material circumstances such as work and home environment, as well as psychological and behavioral factors. Social cohesion and social capital bridge the gap between structural and intermediary determinants. They describe the willingness of people in a community to cooperate for the greater good.
Around 1830, a french physician named Louis Villerme correlated morality by the district in Paris. The result showed a correlation between death and the rate of poverty in the district. The Whitehall study was a prospective cohort study which studied mortality in British civil servants in 1967. The result showed at each occupational grade, health status was higher and mortality was lower. This is apparent in most industrialized countries, but the inverse was true in developing countries. In Nigeria, for example, obesity is found more commonly in the upper classes.
Ultimately, it is only through collective action we can bring problems to light and determine a solution through social policy. In 1842 Sir Edwin Chadwick published a paper called "Report into Sanitary Conditions of the Labouring Population of Great Britain" which concluded life expectancy was higher in the countryside than in towns. He argued the solution was not more doctors, but civil engineers to improve sanitary conditions in the city. These were eventually brought to parliament and legislation was passed to reform public health in the UK.
- Nuisances Removal Act (1846) - Gave local justices the power to prosecute landlords for infractions having to do with sanitation.
- Public Health Act (1848) - Created a general board of health that could create local boards and deal with environmental filth.
- The Epidemiological society of London was formed in 1850 to present papers related to public health
- John Snow wrote a paper in 1853 that sparked further reform.
Politics dictate who are provided with services and how the budget is spent. The Organization for Economic Cooperation and Development (OECD) which categorized governments; Social democratic, christian democratic, liberal, and authoritarian conservative/dictatorship. The authors concluded that redistribute polices are positive associated with health outcomes.
Mental Health
In 2015, an estimated 43.4 adults reported having a mental illness. About 25% of US adults have mental illness and nearly 50% will develop one during their lifetime. Mental health is associated with chronic medical diseases such as heart disease, diabetes and obesity. Both intentional (suicide) and unintentional death (car crashes) are 2-6x higher in people with mental illness. Mental health is also greatly influenced by our environment and socioeconomic standing.
Critical periods are windows in which the impact of exposure to stressors and protective factors are heightening and can have long-term effects. These periods include:
- Prenatal/pregnancy
- Early childhood
- Adolescence
- Working and family building years
- Older ages
There are several terms used to determine a person's mental well-being. Well-being is associated with numerous health, job, family, and economic benefits such as self-perceived health, longevity, healthy behaviors, and social connectedness and productivity.
Hardiness is an individual's sense of control, involvement and willingness to change and grow
Acculturation is the psycho-social adjustment and adaptation to a new culture of a person from another culture
Resilience is the process of successful adaptation after trauma
Factors influencing mental health include income, crime, family, and so much more.
Strategies for improving mental health include:
- Surveillance - providing estimates on existing mental illness in a society
- Screening and early identification - about 50% of mental health conditions begin by age 14 and 75% by age 24.
- Preventive intervention - prevention practices for selected at risk youth reduces the biological and psychological risk. Some individuals have genetic predispositions for certain mental illnesses, but environmental factors can contribute (exposure to drugs, poor nutrition or toxins)
- Health promotion - efforts to enhance an individual's ability to achieve developmentally appropriate tasks and a positive sense of self-esteem, well-being, and inclusion
- Building healthy public policy
- Creating physical and social environments supportive of individual change
- Strengthening community action
- Developing personal skills - such as increased self-efficacy and feelings of empowerment
- Reorienting health services to the population and partnership with patients
- Community action - Reduce barriers to accessing qaulity education, adequate mental health care, and improve health outcomes among community members by providing resources and skills, as well as screening and early treatment for mental health and substance abuse.
- Policy interventions - policies and laws that increase access to and quality of education, access to employment opportunities and healthy food, and improve housing standards.

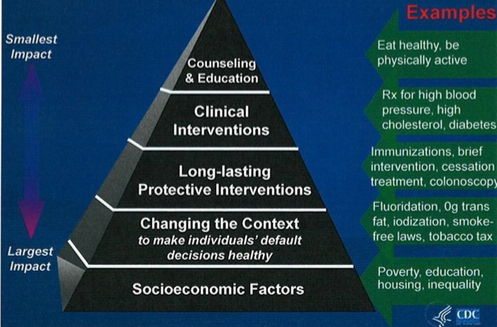
Globalization
The global transportation networks has fostered trade, economic development, and the spread of pathogens to distant locations. Imported foods may lack sanitary safeguards. In many countries globalization lead to an increase in life expectancy starting in the 1950s, however this is accompanied by a increased risk of chronic disease. For example, in the 90's Mexico had an obesity rate of 7%, in 2010 it was 20% this is attributed to the NAFTA. Globalization is also invariably associated with increased energy consumption.
Environmental Health
The environment includes air, water food, products we use, and social, political and economic factors. A framework that connects hazards and adverse outcomes is called the source-exposure-disease conceptual model.